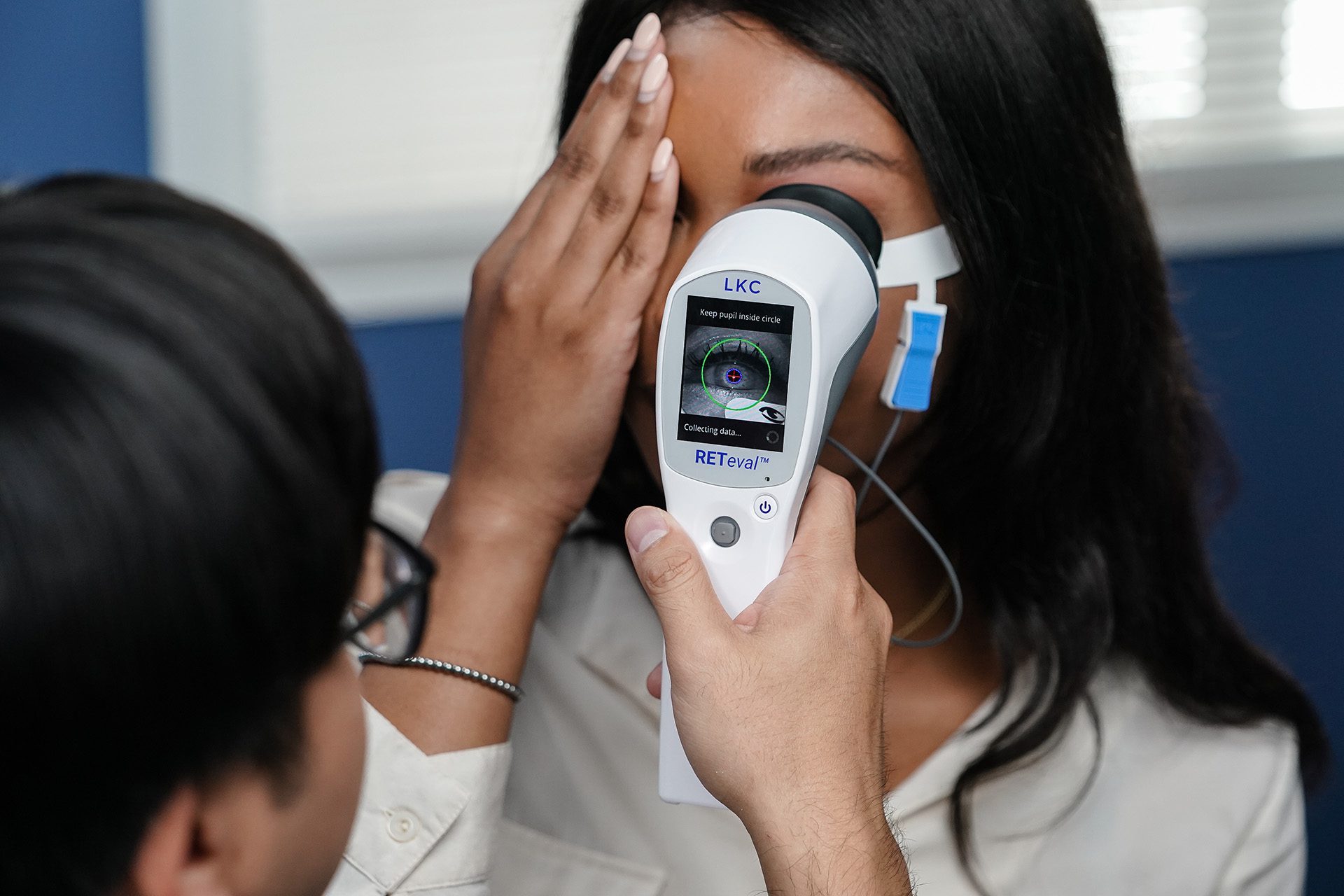
Functional testing is an important complement to structural tests. The RETeval® in particular is a powerful, objective aid in the diagnosis and management of retina and optic nerve diseases, such as diabetic retinopathy and glaucoma.
Why is it necessary to complement structural testing with functional testing?
Dr. Schweitzer: Structural testing gives us a behind-the-scenes look at what’s happening that a patient couldn’t possibly tell us about. Structural tests are important because they show us what’s happening anatomically and we are then able to increase our confidence in a diagnosis if we can match the anatomical changes to the functional changes a patient might be experiencing.
Are visual fields and visual acuity sufficient functional complements to structural testing?
Dr. Bynum: Visual fields and visual acuity are subjective tests that rely on patient feedback. Results are often difficult to obtain and the tests can be very stressful for patients. There are times when, after several minutes of testing, we can’t even use these results. This is why an objective measure of function is so valuable. An ERG test, in particular, provides objective information on the function of the visual system. It gives reliable guidance for medical professionals to manage functional changes that may impact a patient’s vision, typically in advance of structural changes. This is an important feature of ERG testing—it allows us to detect functional stress so that we can anticipate structural damage. Since function is what’s most important to patients and it’s a big red flag for what we are likely to soon see on a structural test, its importance in eye care practices should not be minimized. On the contrary, functional tools like ERG can provide clear answers and allow us to confidently make clinical decisions, particularly when we’re treating common conditions such as diabetic retinopathy and glaucoma.
How does the RETeval change the way you manage diabetic retinopathy in your practice?
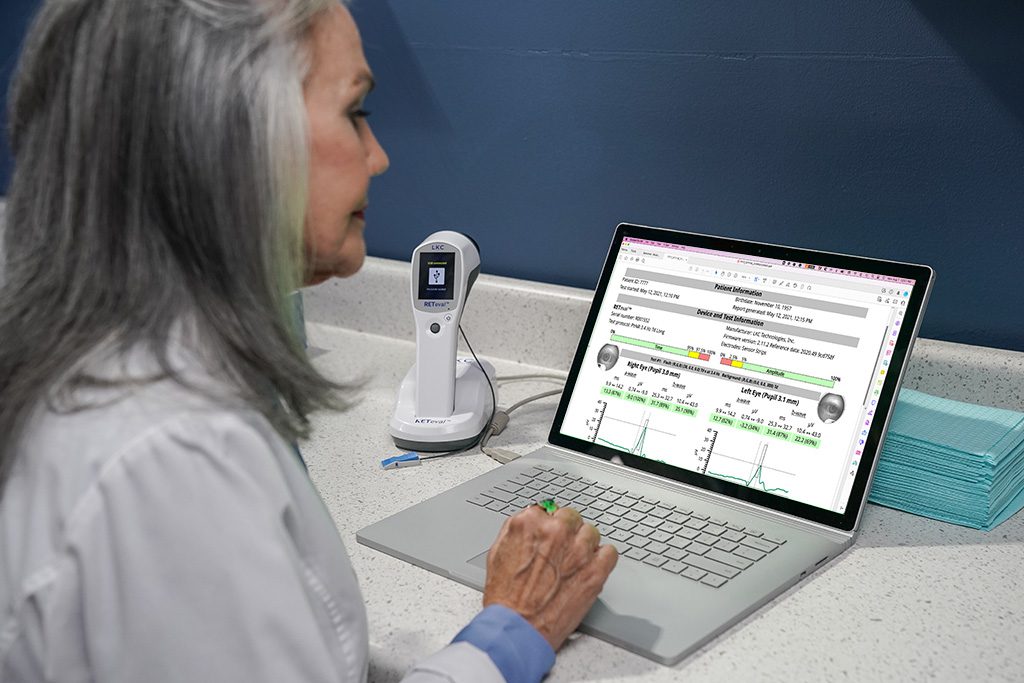
Dr. Gerson: Optometrists rely on the RETevalto diagnose and manage a multitude of ocular conditions, but in my practice, the greatest value is in assessing diabetic retinopathy progression risk. The test is non-invasive and entirely objective, providing a simple score that indicates whether my patient may be in trouble. This is achieved by measuring both retina cell stress and pupil light response. This powerful combination provides a reliable progression risk assessment. It’s also so easy to perform. Many of my colleagues delegate ERG testing to their staff and have a protocol to determine who to pretest before the doctor enters the exam room. It is so simple and quick to perform, that, when I have a patient that I need tested, I usually will just go and grab the hand-held unit and do the test myself. We’re done within a matter of minutes without ever having to move my patient to do it. And, I get immediate results. A score of 23.5 or higher indicates an 11-fold risk of requiring intervention within 3 years,1 which obviously plays a significant role in my clinical decision-making, especially with regard to setting follow-up intervals and appropriately timing referrals.
"Optometrists rely on the RETeval to diagnose and manage a multitude of ocular conditions, but in my practice, the greatest value is in assessing diabetic retinopathy progression risk."
There are so many tests for managing glaucoma. Why should we add ERG?
Dr. Bynum: In short, ERG is one more tool in our arsenal as we try to make sense of a very complicated condition. Despite the availability of modern tools, 50% of true glaucoma patients remain undiagnosed and 50% of glaucoma patients are over-treated.2 Tests such as perimetry and OCT imaging are standard of care, but are all too often hampered by media opacities (imaging for cup-to-disc-ratio), unspecific testing methods (IOP), or are subjective and bothersome to complete (visual field test). For glaucoma diagnosis and management using ERG, several parameters are given as the disease itself is com-plex and the condition is often challenging to diagnose and manage.
How does the RETeval change the way you manage glaucoma in your practice?
Dr. Schweitzer: Since early diagnosis is essential to preserve vision loss from further degeneration of ganglion cells, the RETeval PhNR (Respuesta Fotópica Negativa) test is useful during some glaucoma checks. PhNR stands for photopic negative response and is an electroretinographic test for analyzing how the ganglion cells function. During the PhNR test with full-field flash ERG, the retina is illuminated with a red flash on blue back-ground under light-adapted conditions. The PhNR response from ERG is described by a time (implicit time) and amplitude. A delayed time generally indicates cell stress, while a lower amplitude indicates cell death. The RETeval PhNR test objectively measures the ganglion cells function by evaluating the electrical activity of the cells to a light stimulus. Knowing about the function of the ganglion cell assists in helping me make a more confident assessment of risk, detection, and management of glaucoma.
About the Authors
Frances Bynum, OD,
Northwest Tennessee Eye Clinic (Martin, TN)
Jeffry Gerson, OD, FAAO
Grin Eye Care (Olathe, KS)
Justin Schweitzer, OD, FAAO
Vance Thompson Vision (Sioux Falls, SD)
Translational Vision Science & Technology August 2020, Vol.9, 40. doi:https://doi.org/10.1167/tvst.9.9.40
Nayak BK, Maskati QB, Parikh R. The unique problem of glaucoma: under-diagnosis and over-treat-ment. Indian J Ophthalmol. 2011;59 Suppl(Suppl1):S1-S2. doi:10.4103/0301-4738.73677
Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Substance Tables:
The table below lists substances which may be contained within LKC’s RETeval and RETevet products. Substances listed as Type 1 are within permissible levels in one or more of LKC’s products. Substances listed as Type 2 are used in the production of some components used in LKC products and may be present at trace levels, but are typically destroyed during processing.