Is ERG Needed if You Have Access to a Good Structural Imaging Device?
By Timothy Earley, OD, Justin Schweitzer, OD, FAAO, Julie Rodman, OD, MSc, FAAO, Steve Ferrucci, OD, FAAO, Nate Lighthizer, OD, FAAO, and James Thimons, OD, FAAO.
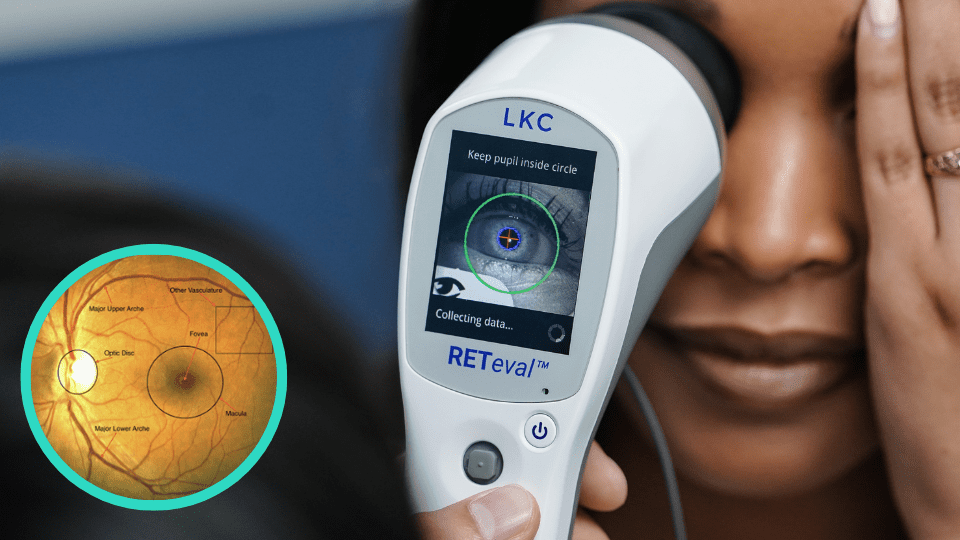
Dr. Earley: Diabetic retinopathy is a chronic, progressive disease, which means we can detect it before it becomes advanced disease. This is best achieved using both structural and functional testing. Electroretinography (ERG) tips us off to functional changes that may impact a patient’s vision—typically in advance of structural changes. This is an important feature of ERG testing—it allows us to detect functional stress so that we can anticipate structural damage. In studies comparing the ability of ERG and structural imaging to evaluate sight-threatening diabetic retinopathy, ERG outperformed traditional imaging at predicting which patients would likely need subsequent medical intervention. 1,2
Dr. Schweitzer: Structural testing gives us a behind-the-scenes look at what’s happening that a patient couldn’t possibly tell us about. Structural tests are important because they show us what’s happening anatomically, and we are then able to increase our confidence in a diagnosis if we can match the anatomical changes to the functional changes a patient might be experiencing.
Dr. Rodman: Early detection of retinal abnormalities is a critical step in preventing vision loss. Importantly, functional loss may precede identifiable structural damage when using an objective test like ERG. Also, it’s important to recognize that, because diabetic retinopathy is a neurovascular disease, retinal function doesn’t always align with structure, which is why functional and structural tests should be used in tandem.
“In studies comparing the ability of ERG and structural imaging to evaluate sight-threatening diabetic retinopathy, ERG outperformed traditional imaging at predicting which patients would likely need subsequent medical intervention.”
Dr. Ferrucci: Beyond diagnosis, ERG also helps us make referral decisions. Traditionally, we base referral on disease severity and presence or absence of diabetic macular edema (DME) as identified using structural tests. But careful consideration of functional abnormalities is important too. Functional tests can offer clear guidance, provided an objective measure like ERG is used. In fact, functional loss alone (provided it’s measured objectively) may be sufficient reason to increase exam frequency or make a referral.
Dr. Lighthizer: Diabetic retinopathy is a puzzle that we put together over time, using all the tools at our disposal to keep our patients safe. ERG is one such tool. It can be used as a baseline throughout the patient’s disease journey in optometric practice. The RETeval® DR Score can guide the patient’s follow-up schedule as well as referral decisions. A score of 23.4 or higher indicates an 11-fold risk of requiring medical intervention within 3 years. 3
Dr. Thimons: Combining structural and functional information provides better results. Electroretinography objectively evaluates the functional abnormalities of the retina, while structural imaging shows the anatomy of the retinal tissue. While both functional and structural assessments have their benefits, functional changes generally appear well before structural changes. In studies comparing ERG and structural imaging’s abilities to evaluate sight-threatening diabetic retinopathy, RETeval ERGs outperformed the traditional imaging techniques in predicting which patients would later need medical intervention. 4,5
Authors
Timothy Earley, OD
Medina Vision and Laser Center
Medina, OH

Justin Schweitzer, OD, FAAO
Vance Thompson Vision
Sioux Falls, SD

Julie Rodman, OD, MSc, FAAO
Nova Southeastern University
Fort Lauderdale, FL

Steve Ferrucci, OD, FAAO
Sepulveda VA Medical Center
Sepulveda, CA

Nate Lighthizer, OD, FAAO
Northeastern State University
Tahlequah, OK
James Thimons, OD, FAAO
Ophthalmic Consultants of Connecticut
Fairfield, CT
1 Brigell, M.G., Chiang, B., Maa, A.Y. and Davis, C.Q. (2020). Translational vision science & technology, 9(9), 40-40.
2 Al-Otaibi, H., Al-Otaibi, M. D., Khandekar, R., Souru, C., Al-Abdullah, A. A., Al-Dhibi, H., … & Kozak, I. (2017). Translational Vision Science & Technology, 6(3), 3-3.
3 Brigell, M.G., Chiang, B., Maa, A.Y. and Davis, C.Q. (2020). Translational vision science & technology, 9(9), 40-40.
4 Brigell, M.G., Chiang, B., Maa, A.Y. and Davis, C.Q. (2020). Translational vision science & technology, 9(9), 40-40.
5 Al-Otaibi, H., Al-Otaibi, M. D., Khandekar, R., Souru, C., Al-Abdullah, A. A., Al-Dhibi, H., … & Kozak, I. (2017). Translational Vision Science & Technology, 6(3), 3-3.