Detecting and managing diabetic retinopathy (DR) has always centered on structural testing, including dilated fundus examination and, in many cases, OCT. How does ERG further enhance clinical decision-making?
Dr. Rodman:Early detection of retinal abnormalities is a critical step in preventing vision loss. Importantly, functional loss may precede identifiable structural damage when using an objective test like ERG. Also, it’s important to recognize that, because DR is a neurovascular disease, retinal function doesn’t always align with structure, which is why functional and structural tests should be used in tandem.
Dr. Earley:DR is a chronic, progressive disease, which means we can detect it before it becomes advanced disease. This is best achieved using both structural and functional testing. ERG tips us off to functional changes that may impact a patient’s vision — typically in advance of structural changes. This is an important feature of ERG testing—it allows us to detect functional stress so that we can anticipate structural damage. In studies comparing the ability of ERG and structural imaging to evaluate sight-threatening DR, ERG outperformed traditional imaging at predicting which patients would likely need subsequent medical intervention.1,2
Dr. Ferrucci:Beyond diagnosis, ERG also helps us make referral decisions. Traditionally, we base referral on disease severity and presence or absence of DME as identified using structural tests. But careful consideration of functional abnormalities is important too. Functional tests can offer clear guidance, provided an objective measure like ERG is used. In fact, functional loss alone (provided it’s measured objectively) may be sufficient reason to increase exam frequency or make a referral.
There are other functional measures that can be used in DR management. What makes ERG stand out?
Dr. Earley: First, measuring visual acuity alone is not an appropriate functional measure when managing diabetic eye disease. On the other hand, ERG offers a direct reading of retinal health by measuring the functioning of the retina.
Dr. Rodman: Having an awareness of the functional health of a diabetes patient is so helpful. ERG measures both retina cell stress and, in some units, pupil light response as well. This powerful combination provides a superior progression risk assessment.
Dr. Ferrucci: Functional tools like ERG can provide clear answers and allow us to confidently make clinical decisions. Newer devices are also non-invasive and entirely objective. The RETeval device even provides a simple score that indicates whether or not a diabetes patient is in trouble.
"In studies comparing the ability of ERG and structural imaging to evaluate sight-threatening DR, ERG outperformed traditional imaging at predicting which patients would likely need subsequent medical intervention."
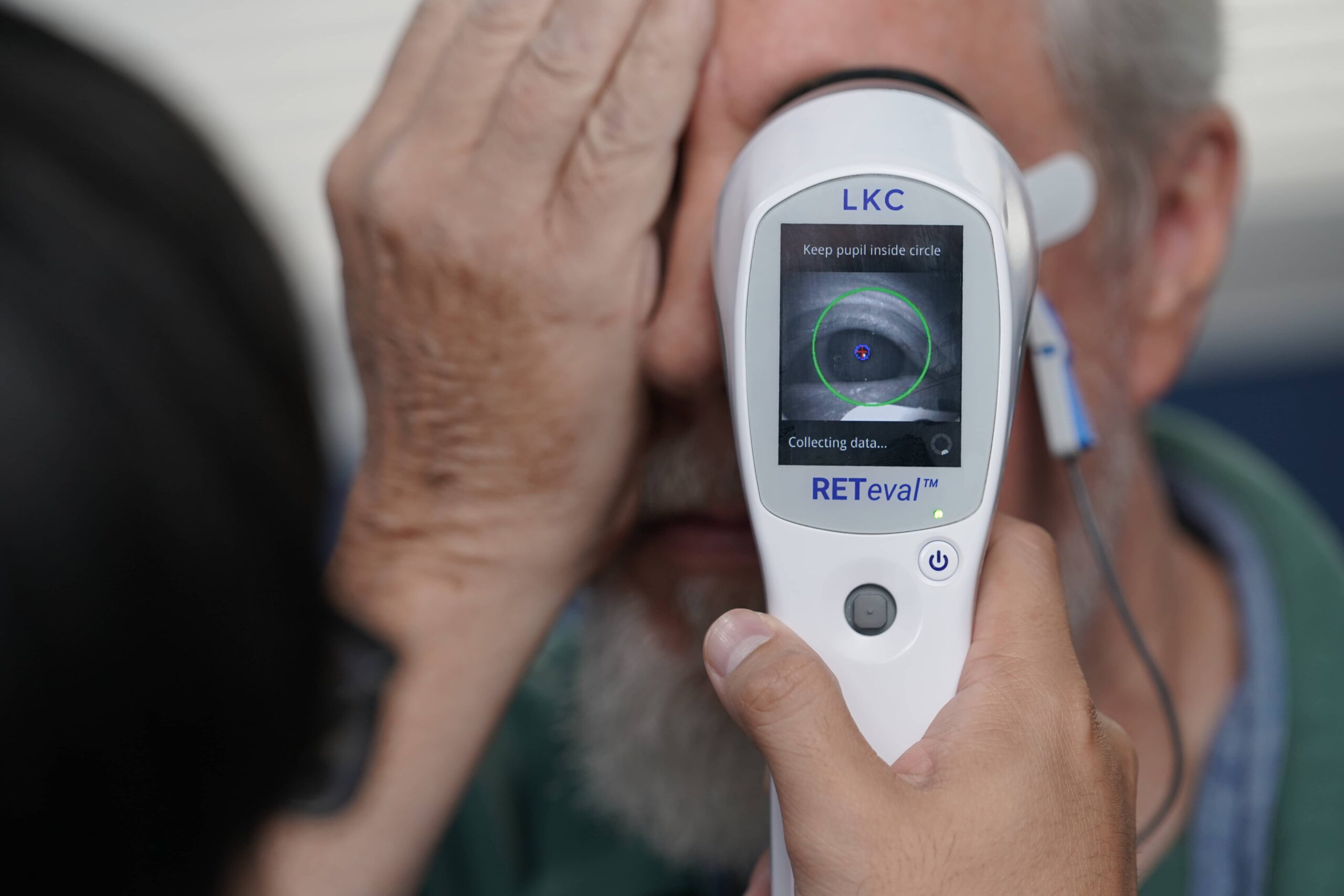
How is the RETeval® device different compared to other ERG technologies?
Dr. Ferrucci: O teste PhNR do RETeval device by LKC Technologies is the only FDA-cleared, portable, battery-operated, non-mydriatic ERG testing instrument on the market in the US. It has skin rather than corneal electrodes, adjusts for pupil size in real time, and doesn’t require dilation.
Dr. Rodman: O teste PhNR do RETeval is unique in that it offers a DR Assessment Protocol that provides a superior risk assessment for progression. As diabetic patients worsen into moderate and severe nonproliferative disease, it may become challenging to determine the best time to refer to a retinal specialist. With the RETeval DR Assessment, you simply check the score. A score of 23.5 or higher indicates an 11- fold risk of requiring intervention within 3 years.1
Dr. Earley: Em uma avaliação da capacidade do RETeval’s ability to evaluate diabetic retinopathy, the advantages included earlier detection of retinal dysfunction, lower investment costs, and less required subjective photo-reading knowledge compared to traditionally-used imaging techniques. In short, the test allows for earlier detection of retinal dysfunction at a lower cost and with less knowledge than is required with traditional imaging.3
Many optometric practices are struggling with staffing shortages that make adding more tests challenging. Is implementing the RETeval device practical in offices that are already stretched thin?
Dr. Rodman: Grading diabetic retinopathy is not easy or fast, but the ERG component is the exception. This is one part of the exam that’s simple and can easily be delegated.
Dr. Earley: A technician can perform a RETeval exam in both eyes within minutes,3 and patients don’t get frustrated because it’s completely objective. It’s also great for the doctor because the device provides immediate results.
Dr. Ferrucci: By adding the DR Score to the chart, I have an excellent baseline for future visits, which saves time while providing straightforward documentation that all the pieces of the clinical and coding puzzle fit together appropriately.
Al-Otaibi, H., Al-Otaibi, M. D., Khandekar, R., Souru, C., Al-Abdullah, A. A., Al-Dhibi, H., … & Kozak, I. (2017). Translational Vision Science & Technology, 6(3), 3-3.
Zeng, Y. et al. (2019). British Journal of Ophthalmology 103, 1747–1752.
Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Substance Tables:
The table below lists substances which may be contained within LKC’s RETeval and RETevet products. Substances listed as Type 1 are within permissible levels in one or more of LKC’s products. Substances listed as Type 2 are used in the production of some components used in LKC products and may be present at trace levels, but are typically destroyed during processing.