Estudo de Caso
A Family Affair: ERG-Guided Care for a Married Couple
by Amanda Legge, OD
A married couple, both of whom have a history of diabetes, presented on the same day for routine comprehensive vision examinations. Neither patient reported any new vision complaints, and their eyesight was easily correctable to 20/20 with minimal change in refractive error.
Watch the video of Dr. Legge presenting her case or review the case below.

Desagio
Determining Severity of Disease

Diagnóstico
Retinopatia Diabética

Testing Protocol
DR Assessment
Patient 1: The Wife
Patient History
The wife is a 72-year-old white female with a systemic history that includes insulin-dependent diabetes mellitus (IDDM), hypertension and hypercholesterolemia. Her systemic medications consisted of semaglutide, insulin, lisinopril-hydrochlorothiazide and pravastatin. Her most recent A1c score was 7.5%.
Her ocular history included cataract surgery OU and proliferative diabetic retinopathy (PDR). The latter had been treated with panretinal photocoagulation (PRP) and anti-VEGF injections, and she had not required treatment for more than five years.
Why Was the ERG Test Performed?
I performed an ERG for two reasons. First, as I would expect, earlier fundus photos revealed significant retinal damage following PRP (Figure 1). Second, I would expect the peripheral retinal damage to begin to affect overall retinal function.
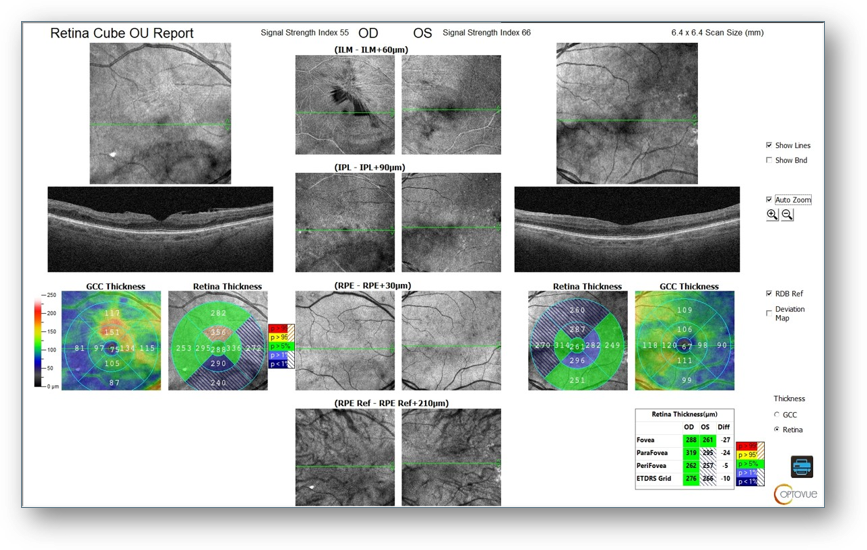
There was also evidence of ongoing vascular changes on OCT-A, including an irregular/asymmetric foveal avascular zone and capillary dropout (Figure 2) along with moderate ERM OD with central microaneurysms on OCT (Figure 3). As such, I wanted to monitor for progression that might require additional intervention.
Figure 1: Fundus
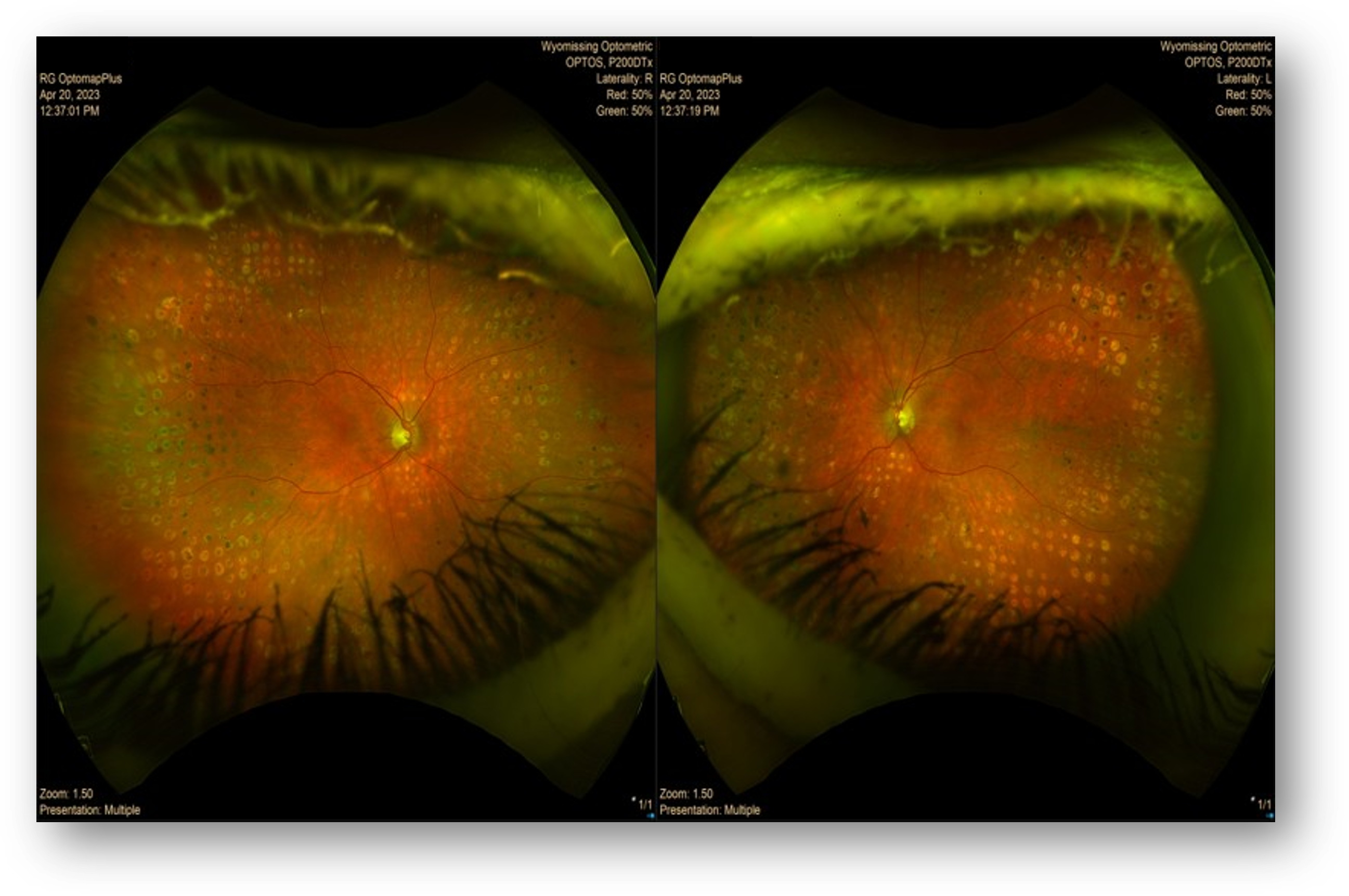
Figure 2: OCT-A
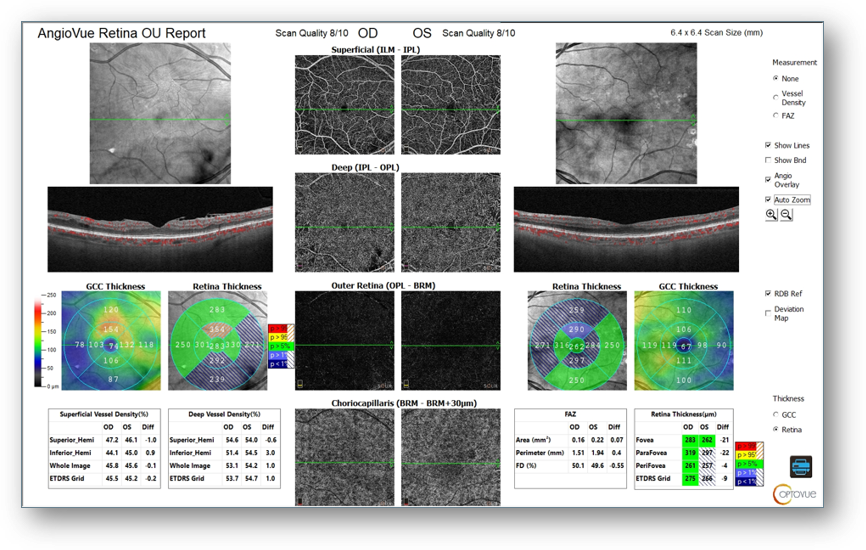
Figure 3: OCT
What Were the ERG Findings?
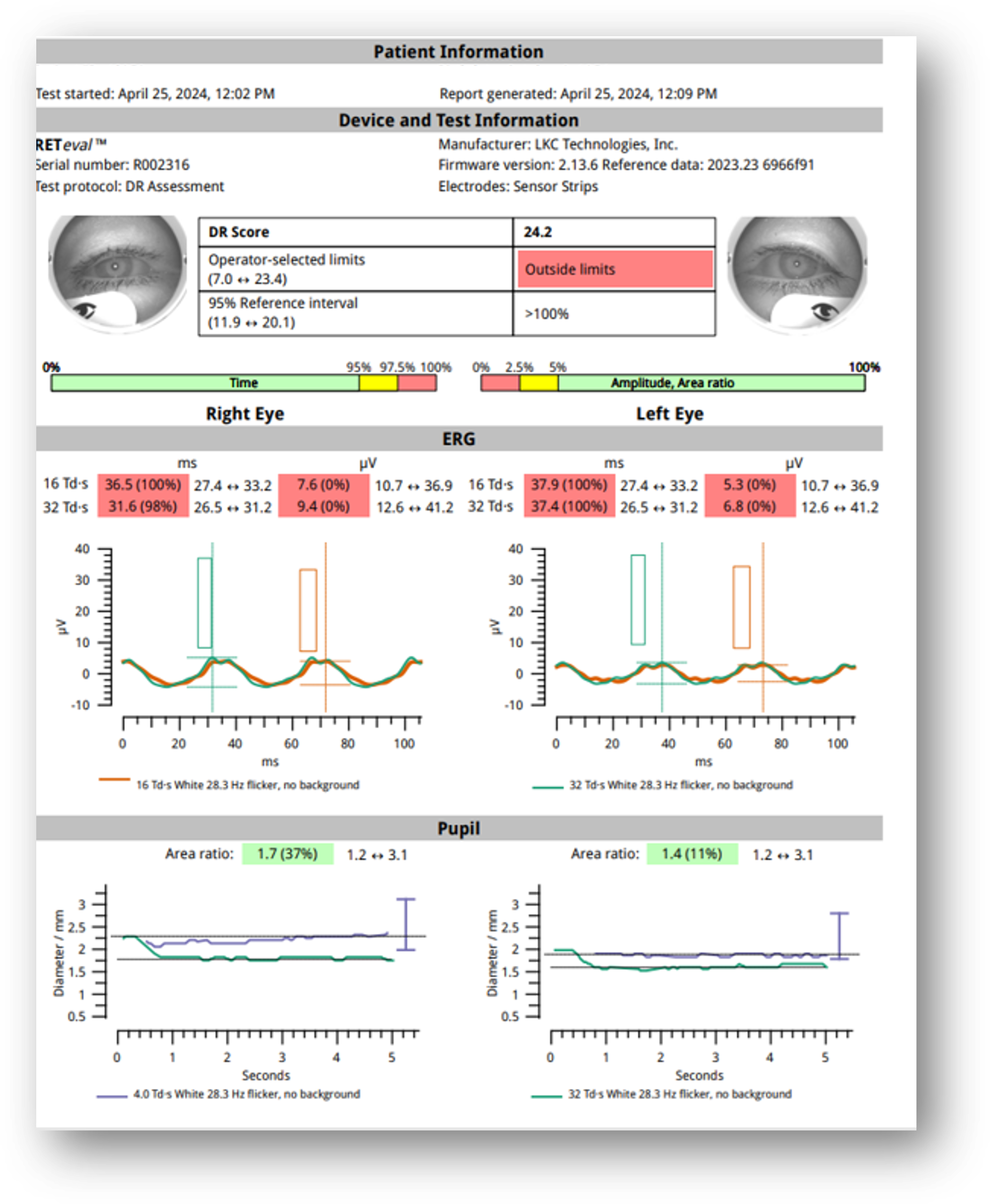
The patient record included an ERG collected the year prior, with a DR Score of 24.5 with slow implicit times and weak amplitudes OU (Figure 4). My repeat testing at this visit revealed a DR Score of 24.2. I diagnosed the condition as inactive PDR OU. Although she remains asymptomatic, with no statistically significant change in her DR Score, she remains in the high-risk category and will likely require intervention within the next three years.
Figure 4: ERG 2023
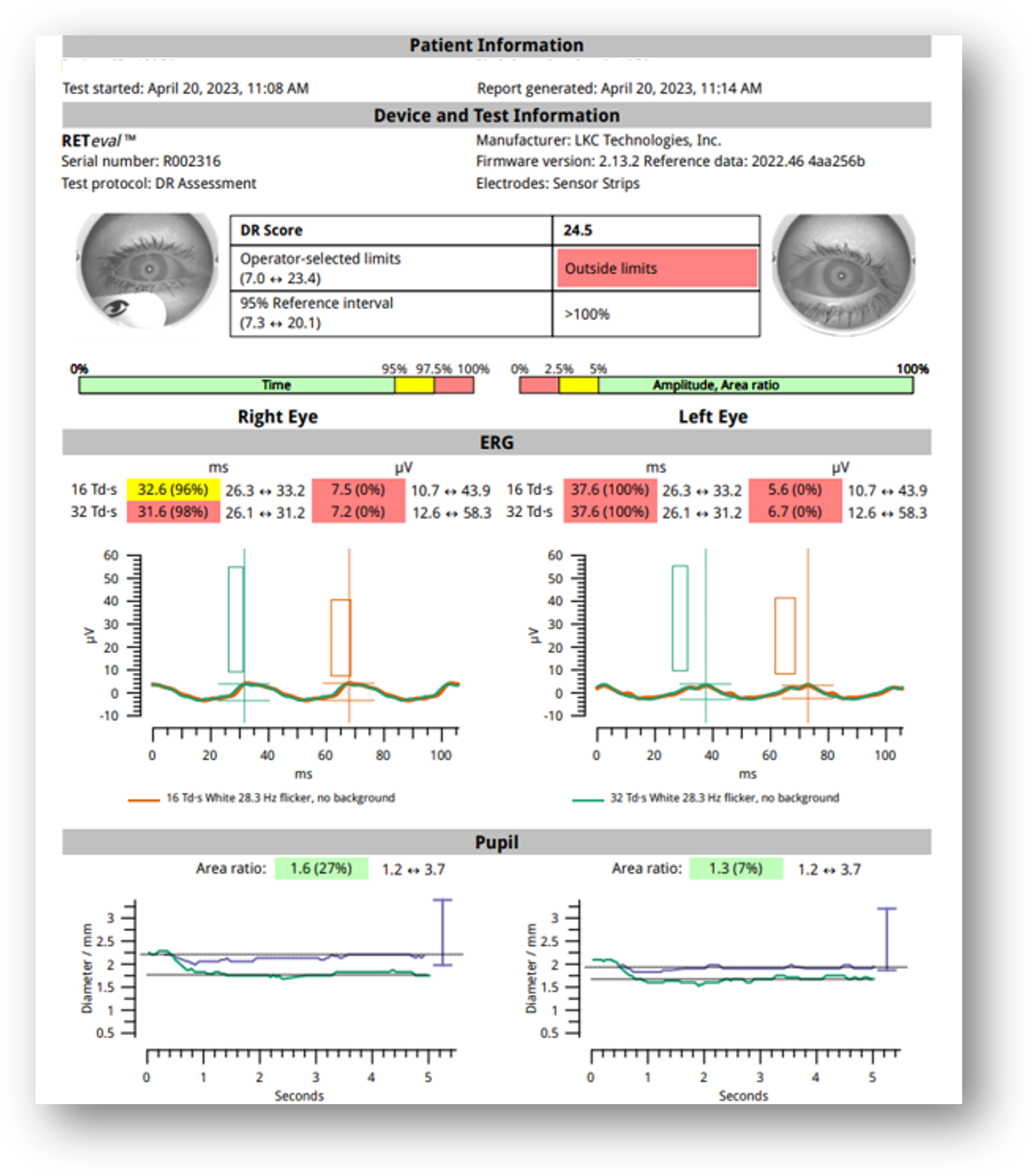
Figure 5: ERG 2024
How Did the ERG Impact Next Steps?
The ERG confirmed abnormal retinal function consistent with her history of advanced diabetic retinopathy. Although her condition had remained anatomically stable, her persistently high DR Score prompted closer follow-up. I now monitor her every six months, and her care plan emphasizes tighter glycemic control.
Patient 2: The Husband
Patient History
The husband is an 80-year-old white male whose systemic history included IDDM, hypertension, hypercholesterolemia, dementia, and hypothyroidism. His medications included levothyroxine, insulin, glimepiride, metoprolol, and tirzepatide. His most recent A1c was 7.4%; however, his blood glucose had been running higher than average over the previous six weeks owing to a pharmacy backorder of the medication.
His ocular history also included cataract surgery OU and small hard drusen, but he had no history of diabetic retinopathy.
Why Was the ERG Test Performed?
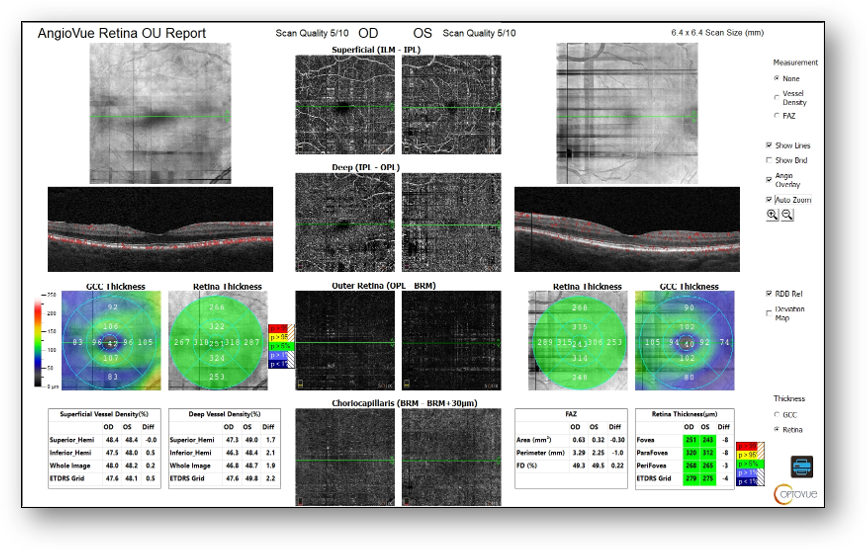
Fundus images showed small hard drusen throughout both maculae but no diabetic retinopathy (Figure 6). OCT revealed small drusen OU, mild ERM OD, and no diabetic retinopathy or macular edema (Figure 7). Notably, abnormal and asymmetric FAZ and capillary dropout OD > OS were found on OCT-A (Figure 8). These structural findings, combined with the patient’s poorly controlled diabetes secondary to medication unavailability were cause for concern and prompted me to perform ERG.
Figure 6: Fundus

Figure 7: OCT
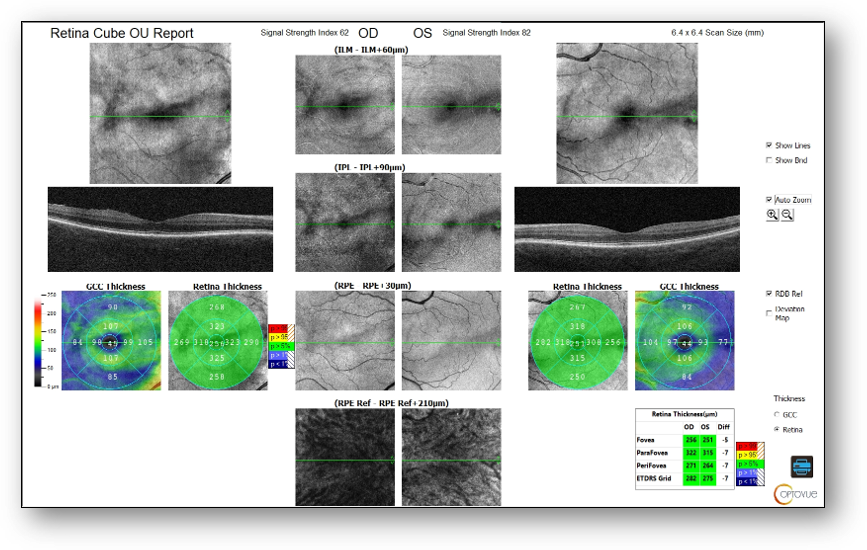
Figure 8: OCT-A
What Were the ERG Findings?
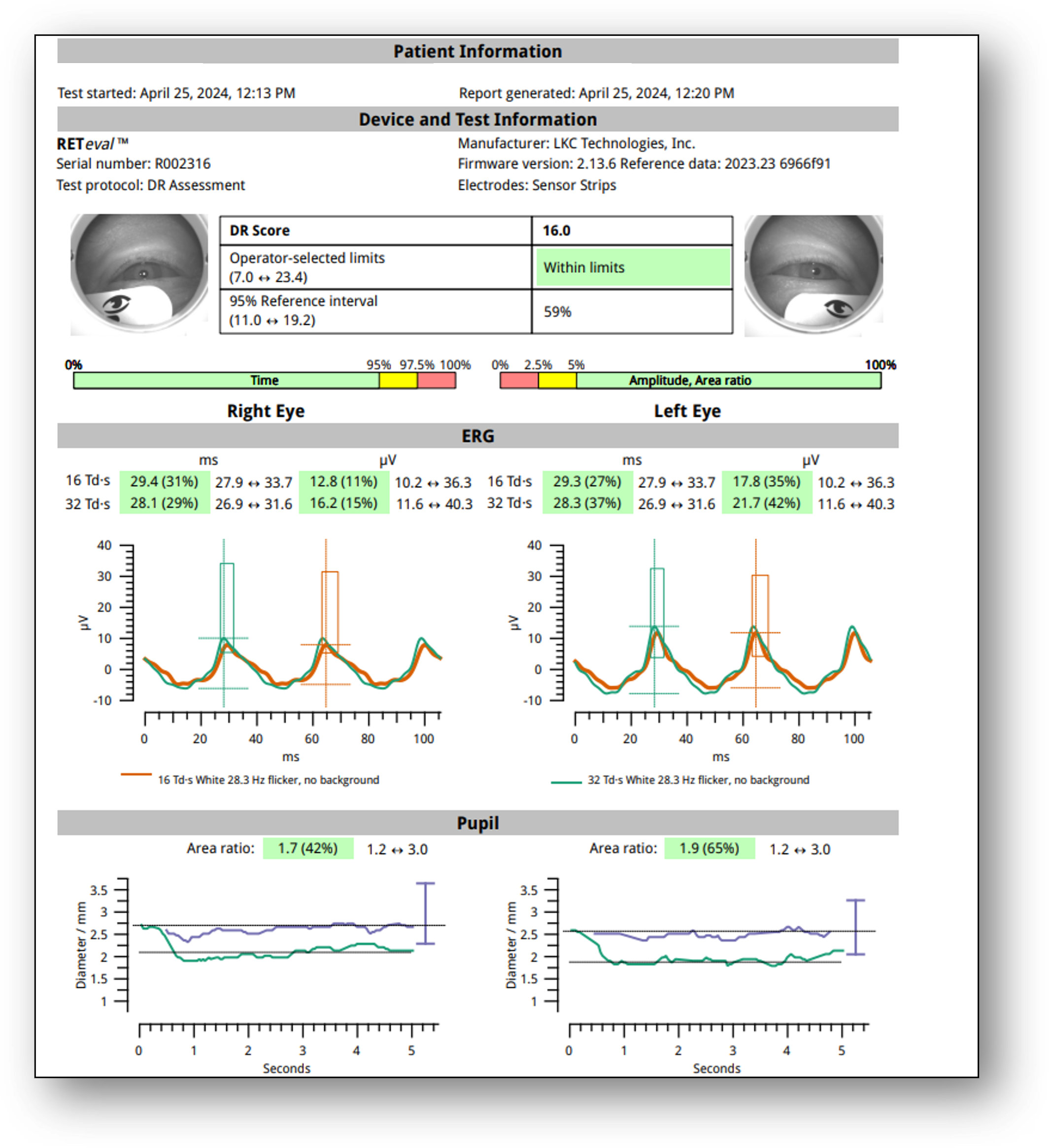
ERG testing showed a DR Score of 16.0, which is well within normal limits (Figure 9). Additionally, I noted only mild asymmetry in amplitude (OS > OD). These results were reassuring given the patient’s systemic risk factors.
Figure 9: ERG
How Did the ERG Impact Next Steps?
The ERG allowed me to confidently reassure the patient that his retinal function remained normal, despite recent blood glucose fluctuations. I counseled him on the importance of regaining metabolic control to avoid future complications and communicated my findings to his primary care physician for coordinated management.
Summary
These paired cases highlight the value of ERG in assessing and monitoring retinal function in patients with diabetes. For the wife, ERG confirmed high functional risk despite long-term anatomical stability, justifying more frequent monitoring. For the husband, ERG reassured both me and the patient that retinal function was normal despite systemic challenges.
This case was billed using E11.3493 for the wife and H35.013, noted arteriole narrowing and AV nicking, for the husband.
Why We Use RETeval
We use RETeval because it enables us to watch progression, or the potential for progression, with functional data. It is an ideal supplement to the standard fundus and OCT imaging we implement to track retinal health and risk.
Practice Protocol
We have been using RETeval since July of 2022. We utilize it primarily in patients who have diabetic retinopathy and glaucoma. However, we also have found it to be valuable for evaluating patients who have unexplained vision loss in the absence of identifiable structural findings, as well as in patients with inherited retinal disease.
Amanda Legge, OD
Wyomissing Optometric Center
Dr. Amanda Legge practices at Wyomissing Optometric Center in Wyomissing, PA, where she provides primary eye care with a special interest in retinal diseases. She is professionally recognized for her expertise in diagnosing and managing age-related macular degeneration and inherited retinal diseases, and frequently lectures to fellow optometrists on retinal disease and eye care.