In your opinion, are there clear protocols in optometry for managing patients with diabetes?
Dr. Chous: Unfortunately, there are not. This unmet need in our profession creates a lot of variation in patient care and, ultimately, in patient outcomes.
Dr. Wood: I couldn’t agree more. We absolutely need some basic guidelines and concrete strategies that standardize how we meet this growing patient need.
Dr. Hitchmoth: Some would argue that a dilated fundus exam and visual acuity check tick the box, but in my experience, it’s not enough. In many cases, these basics don’t give us the confidence to say that we’re doing all we can for patients.
What more can optometrists do without putting too much strain on their practices and staff?
Dr. Chous: I’ve been giving this a lot of thought this past year and I think it’s helpful to look at the fundamentals of diabetic retinopathy management across broad categories. We need to 1) detect, 2) grade, 3) assess risk, 4) manage, and 5)support.
Dr. Wood: As basic as this sounds, it can be a tall order. Grading and assessing risk require a lot of skill and time, and are arguably subjective.
Dr. Hitchmoth: Subjectivity is a big part of the problem. What’s needed is a blueprint that provides some guidance on putting the puzzle pieces together.
"It’s helpful to look at the fundamentals of diabetic retinopathy management across broad categories. We need to 1) detect, 2) grade, 3) assess risk, 4) manage, and 5) support."
If you looked at these five categories one by one, starting with detection, what would you put forward as essential practice guidelines?
Dr. Hitchmoth: I would start by saying that we need to approach diabetic retinopathy as a chronic progressive disease.
Dr. Wood: Exactly. And being a chronic progressive disease implies that you can detect it before it becomes advanced disease. The question is, how do we do this?
Dr. Chous: To begin, we need to use both structural and functional testing. OCT-A is a real game changer in structural testing. And on the functional side, although the standard of care for the assessment of vision loss due to diabetic retinopathy is high-contrast visual acuity, evidence shows it is insufficient.
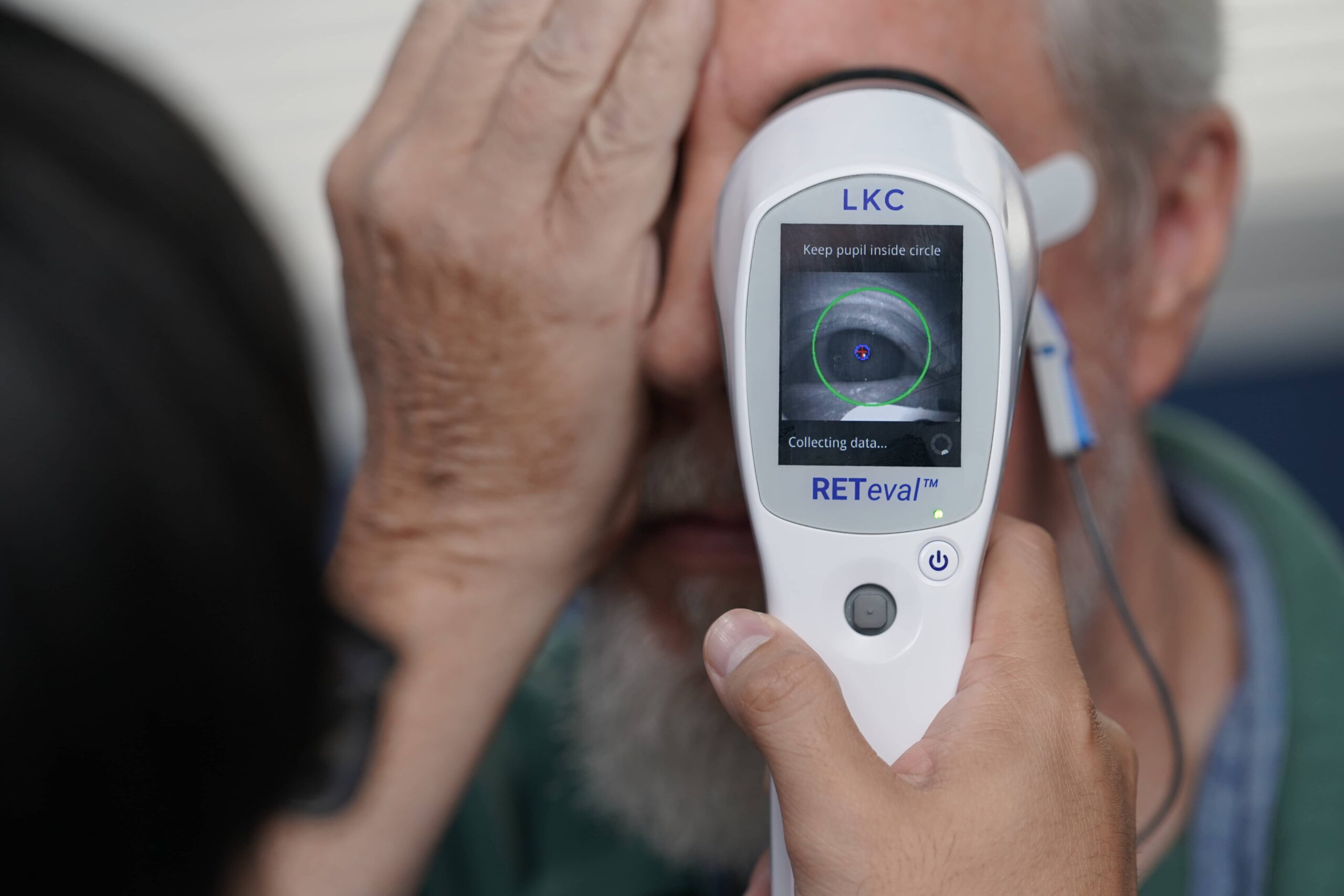
Dr. Hitchmoth: I advocate for electro-diagnostic testing (ERG), preferably utilizing the additional measure of pupillometry, as in the DR score offered by the RETeval® device, since this provides a direct reading of retinal health.
In the grading category, what do you recommend?
Dr. Chous: At the most basic level, diabetic retinopathy should be graded at the time of diagnosis and at each subsequent visit. Charting is also important and should include a record of structural retinal damage.
Dr. Wood: Quantifying retinal cell function is likewise essential. For this, I use ERG. ERG is a measure of the function of the retina, the health of the cells, and the risk of disease progression that is fast and easy to perform using the handheld RETeval device.
How do you assess risk?
Dr. Chous: Here again, both structural and objective functional measures are crucial, and the two may not align, which makes things tricky.
Dr. Hitchmoth: We may be used to seeing structure first when we rely on visual acuity, but when using objective tests such as ERG, functional loss can precede identifiable structural damage. That’s important information that plays a role in how I monitor and manage the patient moving forward.
Do you have any guiding principles in terms of management?
Dr. Chous: The time between retinal examinations depends on risk assessment, but no matter how severe or early the disease is, I strongly believe that multi-disciplinary resources are required to manage all diabetic retinopathy patients.
Dr. Hitchmoth: Good nutrition is also essential and is something we should emphasize with our patients.
Finally, in terms of support, what can optometrists do to help patients who have diabetes?
Dr. Wood:First and foremost, we need to provide comprehensive patient education and strategies to help prevent disease progression.
Dr. Chous: To that end, it’s important to emphasize the asymptomatic nature of DR at its earliest, most treatable levels of severity and encourage patients to achieve individually optimized metabolic control in concert with their diabetes physicians.
Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Substance Tables:
The table below lists substances which may be contained within LKC’s RETeval and RETevet products. Substances listed as Type 1 are within permissible levels in one or more of LKC’s products. Substances listed as Type 2 are used in the production of some components used in LKC products and may be present at trace levels, but are typically destroyed during processing.