
By Paul Chous, MA, OD, FAAO, Ansel Johnson, OD, and Julie Rodman, OD, MSc, FAAO
Originally published in the August 2023 issue of Review of Optometry.
Dr. Johnson: A Diabetic Retinopathy Taskforce was formed last year, and we are currently finalizing a consensus document that will spell this out. The approach includes five pillars. In short, optometrists need to 1) detect, 2) grade, 3) assess risk, 4) manage and 5) support.
Dr. Chous: As members of that task force, I think I speak for the three of us when I say that, even from our very first meeting, we knew that grading and risk assessment are pain points in optometry. It tends to be highly subjective, can take a lot of time and skill, and therefore needed to be a central focus of our initiative.
Dr. Chous: We all unanimously agreed that we need to grade diabetic retinopathy at the time of diagnosis and at each subsequent visit. Furthermore, we should chart structural retinal damage and quantify retinal cell function.
Dr. Rodman: Most of us already conduct grading at some level and note it in the chart. But the quantification of retinal cell function is where we see the most significant opportunity loss. Although both structure and function are useful, functional changes generally appear well before structural ones. In studies comparing the ability of ERG and structural imaging to evaluate sight-threatening DR, ERG outperformed traditional imaging at predicting which patients would likely need subsequent medical intervention.1,2
Dr. Johnson: Importantly, visual acuity alone is not sufficient to assess function.
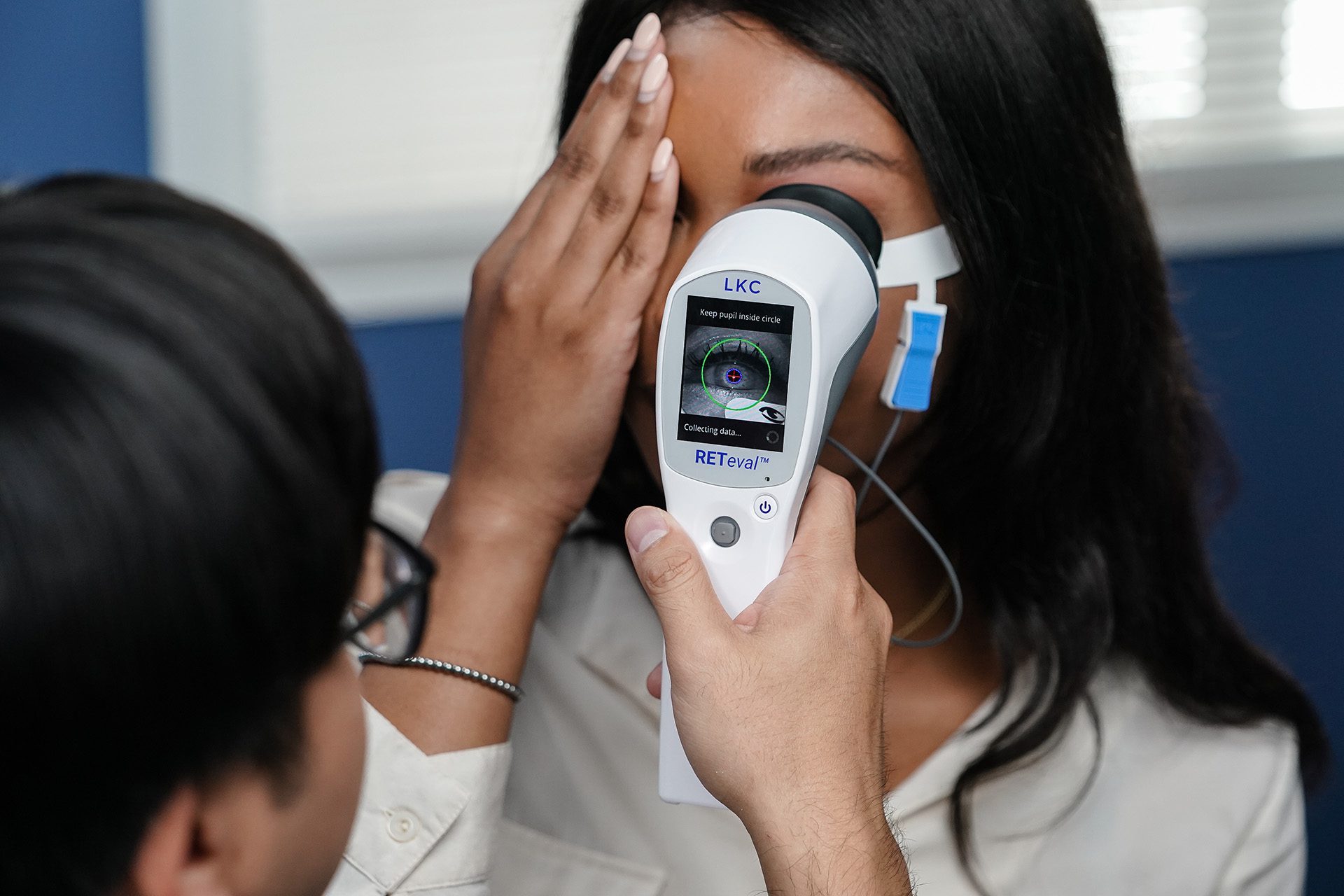
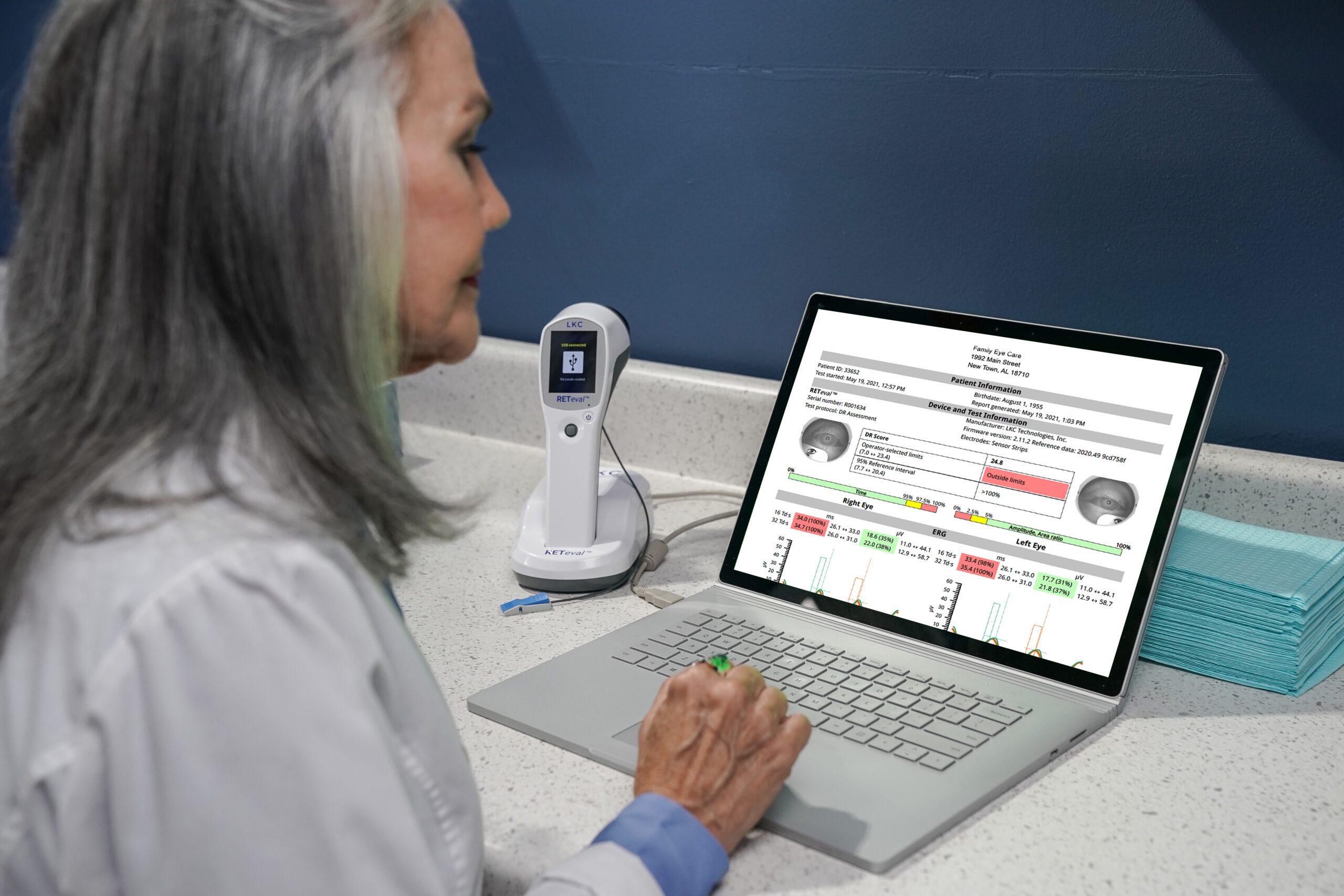
Dr. Johnson: An objective test, such as ERG, is needed. In my practice, we use the RETeval® device. This handheld technology is fast, reliable and easy to perform. It also generates an extremely user-friendly report that’s excellent for charting purposes.
Dr. Rodman: I rely on the RETeval device as well. It streamlines care and gives me peace of mind. It’s easy enough for my technicians to use, coding is straightforward, and the reimbursement is fair.
Dr. Chous: This can be challenging because you want to know where the patient stands in that moment, but generating an answer about risk at a single moment in time isn’t easy because different tests can tell different stories. You have to put the puzzle together to create a portrait of risk.
Dr. Johnson: This is probably the most important reason to look at both structural and objective functional measures because the two may not align and, if one of them raises alarm, we need to keep digging. Having baseline functional and structural assessments can be tremendously valuable.
Dr. Chous: Dilated retinal exams are important, preferably with fundus photography and red-free filtration to detect subtle structural abnormalities, and OCT/OCTA imaging is helpful for future comparison. In terms of the functional risk assessment, initial full-field ERG (ffERG) is recommended for patients with any DR at baseline to establish a comparator if future DR worsening is detected subsequently.
Dr. Rodman: With an objective ERG test, functional signs of loss can predict progression.1,2 Specifically, a RETeval DR Score of 23.4 or higher indicates an 11-fold risk of requiring medical intervention within 3 years.2
Dr. Johnson: This score also can guide the follow-up schedule or referral decision. (See Retinopatia Diabética Monitoring and Referral Guidelines above.)
Chous Eyecare Associates
(University Place, WA)

The Eyecare Institute – Broward
(Fort Lauderdale, FL )
1 Al-Otaibi H, Al-Otaibi MD, Khandekar R, et al. Transl Vis Sci Technol. 2017;6(3):3. doi:10.1167/tvst.6.3.3
2 Brigell MG, Chiang B, Maa AY, Davis CQ. Transl Vis Sci Technol. 2020;9(9):40. doi:10.1167/tvst.9.9.40
![]() Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Substance Tables:
The table below lists substances which may be contained within LKC’s RETeval and RETevet products. Substances listed as Type 1 are within permissible levels in one or more of LKC’s products. Substances listed as Type 2 are used in the production of some components used in LKC products and may be present at trace levels, but are typically destroyed during processing.
RETeval and RETevet Devices
| Substance | CAS # | Type | Listed as causing: |
| Nickel | 7440-02-0 | 1 | Cancer |
| Acrylonitrile | 107-13-1 | 2 | |
| Ethylbenzine | 100-41-4 | 2 | |
| Crystaline Silica | 14808-60-7 | 1 | |
| Lead | 7439-92-1 | 1 | Cancer Developmental Toxicity Male Reproductive Toxicity Female Reproductive Toxicity |
| Methylene Chloride | 75-09-2 | 2 | Cancer Female Reproductive Toxicity |
| Bisphenol A | 80-05-7 | 2 | |
| N-Hexane | 110-54-3 | 2 | Male Reproductive Toxicity |