Dr. Chous: In 2022, I met with several colleagues who share my interest and passion for elevating diabetic eye care in optometry. We all agreed that there was a significant unmet need for concrete strategies to improve optometric management of diabetic eye disease. We formed a task force with a goal of creating actionable, practical guidelines to help address this significant public health issue.
Dr. Lighthizer: After many months of collaboration, we concluded that optometrists can do better for their patients without placing unreasonable burdens on our practices. To that end, the report contains five practical guidelines as well as several proposed strategies for implementation — all of which represent the consensus of the full panel.
Dr. Karpecki: The approach includes five pillars. In short, optometrists need to 1) detect, 2) grade, 3) assess risk, 4) manage and 5) support.
Five Pillars of DR Management
1. DETECT: Approach diabetic retinopathy as a chronic progressive disease. Being a chronic progressive disease implies that you can detect it before it becomes advanced disease. This can be achieved using both structural and functional testing.
2. GRADE: Grade diabetic retinopathy at the time of diagnosis and at each subsequent visit. Chart structural retinal damage and quantify retinal cell function.
3. ASSESS RISK: To assess risk of progression, monitor diabetic retinopathy patients over time using both structural and objective functional measures.
4. MANAGE: Utilize multidisciplinary resources to manage all diabetic retinopathy patients, regardless of disease severity.
5. SUPPORT: Provide comprehensive patient education and strategies to help prevent disease progression.
Your task force agreed that both structure and function are needed when caring for patients with, or at risk for, DR. But what, specifically, do you recommend optometrists use as a functional measure?
Dr. Karpecki: One of the reasons we rely so heavily on advanced structural tools like OCT and OCT-A is because they often show damage before you detect it using conventional examination techniques like fundus biomicroscopy and fundus photography, and certainly visual acuity, which is preserved until late in DR progression. One of the reasons we rely so heavily on OCT is because it provides objective structural measurements, whereas grading DR severity is somewhat subjective. We need better, objective measurements of retinal function to complement structural assessment.
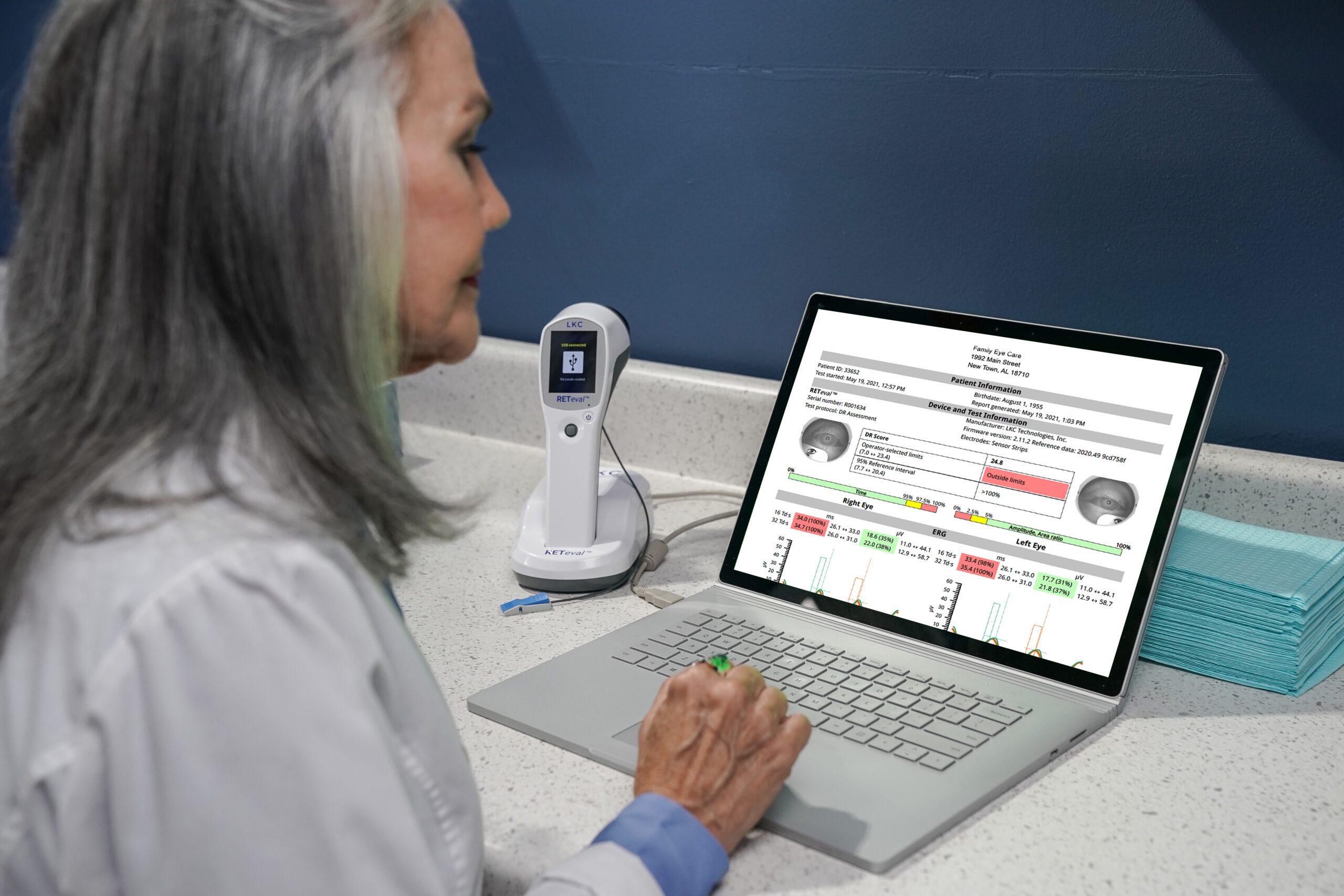
Dr. Lighthizer: Just as we want to see an objective measure of structure, we need an objective measure of function. This is what we get with ERG. With an objective ERG test, functional signs of loss can predict progression.1,2 Better still, it’s faster than refraction. With the handheld RETeval®, you can run a DR protocol test in minutes and have confidence in your management.
Once you’ve established a baseline using ERG, how do you manage and support patients with diabetes in your practice?
Dr. Lighthizer: DR is a puzzle that you put together over time, using all the tools at your disposal to keep your patient safe. ERG is one such tool. It can be used as a baseline throughout the patient’s disease journey in optometric practice. The RETeval DR Score can guide the patient’s follow-up schedule as well as referral decisions. A score of 23.4 or higher indicates an 11-fold risk of requiring medical intervention within 3 years.2
Dr. Chous: The time between retinal examinations depends on risk assessment, but no matter how severe or early the disease is, I strongly believe that multidisciplinary resources are required to best manage all DR patients. Good nutrition is essential and is something we should emphasize with our patients, as well as the importance of preventing hypoglycemia in patients with early DR, an emerging and vastly under-appreciated risk factor for worsening DR.
Dr. Karpecki: Regarding support, it’s important to emphasize the asymptomatic nature of DR at its earlier, most treatable levels of severity and encourage patients to achieve individually optimized metabolic control in concert with their diabetes physicians.
Warning: This product can expose you to chemicals including lead, which is known to the State of California to cause cancer and birth defects or other reproductive harm. For more information go to www.P65Warnings.ca.gov.
Substance Tables:
The table below lists substances which may be contained within LKC’s RETeval and RETevet products. Substances listed as Type 1 are within permissible levels in one or more of LKC’s products. Substances listed as Type 2 are used in the production of some components used in LKC products and may be present at trace levels, but are typically destroyed during processing.