What Type of Functional Testing Do You Prefer for Patients with Diabetes?
By Frances Bynum, OD, Timothy Earley, OD, Steven Ferrucci, OD, FAAO, Dorothy Hitchmoth, OD, FAAO, Ansel Johnson, OD, Nathan Lighthizer, OD, FAAO, Julie Rodman, OD, MSc, FAAO, and Jim Thimons, OD, FAAO.
Are visual fields and visual acuity sufficient functional complements to structural testing?
Dr. Bynum: We need to know as much about function as we do about structure in patients with diabetes; but both visual acuity testing and visual fields are subjective tests that rely on patient feedback. Admittedly, visual acuity measurement is the mainstay of assessing visual function—but it has significant limitations in many patients, including those with diabetes. Results are often difficult to obtain, and the tests can be very stressful for patients. There are times when, after several minutes of testing, we can’t even use visual field results. This is why an objective measure of function is so valuable. An electroretinography (ERG) test provides objective information on the function of the visual system. It gives reliable guidance for medical professionals to manage functional changes that may impact a patient’s vision, typically in advance of structural changes.
Dr. Lighthizer: Just as we want to see an objective measure of structure, we need an objective measure of function. This is what we get with ERG. With an objective ERG test, functional signs of loss can predict progression.1,2
Are ERG devices practical in primary care or do they take up a lot of time and space?
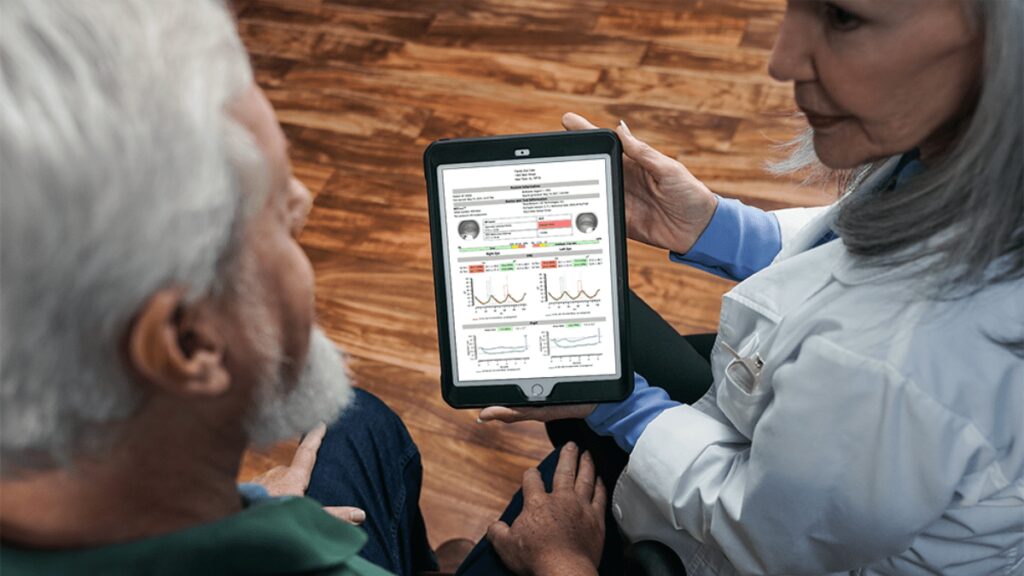
Dr. Earley: That depends on whether you are using an outdated ERG or a next-generation device like the RETeval®, which is what I use to evaluate diabetic retinopathy. The advantages of the RETeval device include earlier detection of retinal dysfunction, lower investment costs, and less required subjective photo-reading knowledge compared to traditionally used imaging techniques. In short, the test allows for earlier detection of retinal dysfunction at a lower cost and with less knowledge than is required with traditional imaging.3
Dr. Lighthizer: Better still, it’s faster than refraction. We can run a RETeval DR Assessment in minutes.
Dr. Thimons: We also use the RETeval device because it’s powerful and fits in the palm of your hand. In fact, it’s the only FDA-cleared, portable, non-mydriatic ERG testing instrument on the market in the US. It is a major departure from traditional electroretinography and represents a technology that has evolved from large, expensive, and complicated to portable, affordable, and easy-to-use and interpret.
Dr. Ferrucci: The RETeval device uses skin rather than corneal electrodes, adjusts for pupil size in real time, and doesn’t require dilation.
What unique information does the RETeval device provide, and how will it make a difference in how I treat my patients?
Dr. Lighthizer: DR is a puzzle that you put together over time, using all the tools at your disposal to keep your patient safe. ERG is one such tool.
Dr. Rodman: The RETeval device is unique in that it offers a DR Assessment protocol that provides a risk assessment for progression. As diabetic patients worsen into moderate and severe nonproliferative disease, it may become challenging to determine the best time to refer to a retinal specialist. With the RETeval DR Assessment, you simply check the score. A score of 23.5 or higher indicates an 11-fold risk of requiring intervention within 3 years.2
Dr. Johnson: This score can guide the follow-up schedule or referral decision.
Dr. Bynum: This is an important feature of ERG testing—it allows us to detect functional stress so that we can anticipate structural damage. Since function is what’s most important to patients and it’s a big red flag for what we are likely to soon see on a structural test, its importance in eye care practices should not be minimized. On the contrary, functional tools like ERG can provide clear answers and allow us to confidently make clinical decisions, particularly when we’re treating diabetic retinopathy.
Dr. Hitchmoth: Early detection of retinal abnormalities is a critical step in preventing vision loss. That’s why the RETeval has become a game changer in how I care for my patients who have diabetes.
Authors

Frances Bynum, OD
Northwest Tennessee Eye Clinic
(Martin, TN)
Timothy Earley, OD
Medina Vision and Laser Center
(Medina, OH)

Steven Ferrucci, OD, FAAO
Sepulveda VA Medical Center
(Sepulveda, CA)

Dorothy Hitchmoth, OD, FAAO
Dr. Dorothy L. Hitchmoth, PLLC
(New London, NH)
Ansel Johnson, OD
Vision Salon Eye Care Associates
(Blue Island, IL)

Nate Lighthizer, OD, FAAO
Northeastern State University
(Tahlequah, OK)

Julie Rodman, OD, MSc, FAAO
Nova Southeastern University
(Fort Lauderdale, FL)
Jim Thimons, OD, FAAO
Ophthalmic Consultants of Connecticut
(Fairfield, CT)