Case study
DR Score Prompts Critical Referral
by Jeffrey Calhoun, OD, FAAO
After years of relying on imaging and average A1C to monitor his patients with diabetes, Jeffrey Calhoun, OD, FAAO, an optometrist in Williamsville, NY, implemented the RETeval handheld ERG as an objective, functional complement to structural assessments. When a patient with well-controlled diabetes came in for an exam, the device’s predictive DR Score revealed significantly compromised retinal function incongruous with the mild retinopathy previously detected, prompting a critical referral to a retina specialist who was able to perform further assessments and uncover severe ischemia.
Watch the video of Dr. Calhoun presenting his case or review the case below.

Challenge
Uncooperative, High-Risk Patient

Diagnosis
Severe Retinal Ischemia

Testing Protocol
DR Assessment
Patient History
A 71-year-old African American female presented for her annual exam. She had a 23-year history of type 2 diabetes mellitus with no other known systemic health problems. She was taking Metformin and Trulicity and did not recall her last A1C test result. She noted that her home blood glucose test was 130 yesterday, but admitted she does not remember to check it every day.
The patient’s record revealed a history of mild non-proliferative diabetic retinopathy (NPDR) OU. She also had a long-standing complaint of difficulty seeing when driving at night, especially in the rain. She declined a cataract referral because she’s afraid of ocular surgery.
Confrontation field testing was full-to-finger counting OD and OS. Extraocular muscle testing revealed full range of motion OD and OS. Cover test demonstrated orthophoria. The patient did have relatively small meiotic pupils that were sluggish upon testing, but pupillary evaluation showed pupils equal, round, and reactive to light and accommodation (PERRLA).
There was no afferent pupillary defect (APD), however manifest refraction did improve vision to a very fuzzy 20/30. Manifest refraction was -0.25 -1.75 x 095 OD and -0.75 -1.25 x 085 OS. Slit lamp examination showed dermatochalasis of the eyelids bilaterally. The conjunctiva and cornea were clear in both eyes, and the anterior chamber was deep and quiet OU. The irides were unremarkable. Significant lenticular changes were observed, with 3+ nuclear sclerosis noted in both eyes, consistent with brunescent cataracts. IOP was 14 mmHg OD and 13 mmHg OS.
In our office, we perform an Optomap on virtually all of our patients, but the patient was unable to keep her eyes open during image capture due to the dermatochalasis. The little we could see showed a couple scattered dot and blot hemes in the retina of each eye (Figure 1).
Figure 1: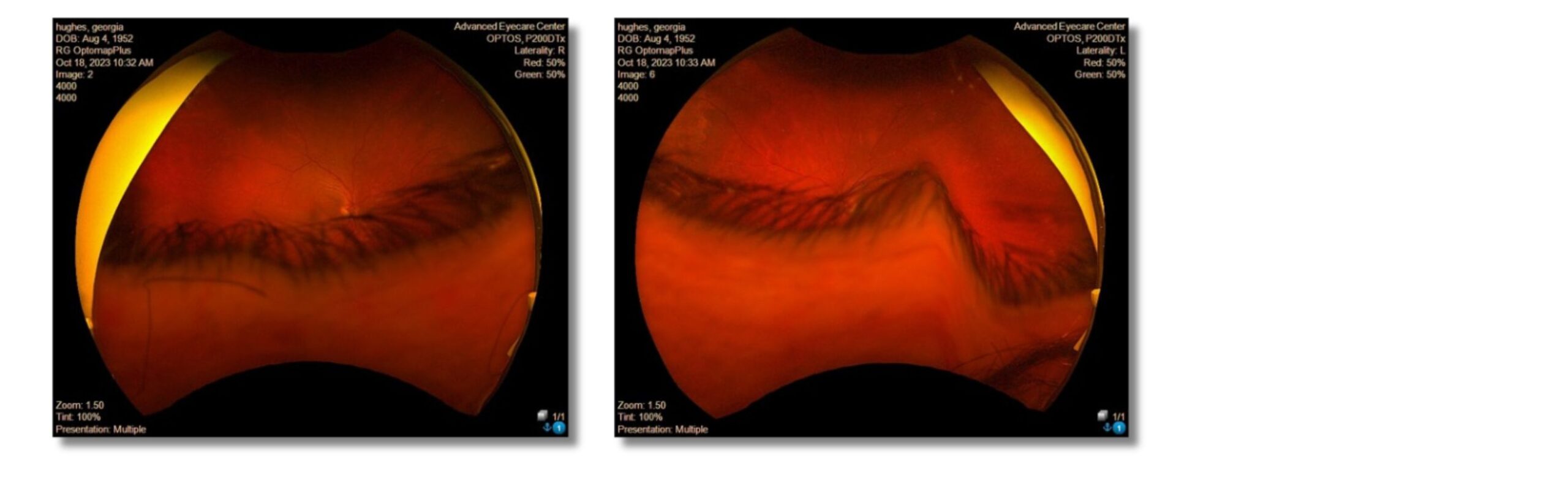
Why Was the ERG Test Performed?
Due to difficult time viewing the retina on the Optomap, as well as the previous history of NPDR, an ERG was performed prior to pupil dilation so that I could get an objective, functional understanding of her diabetic retinopathy and assess risk for progression (Figure 2).
Figure 2:
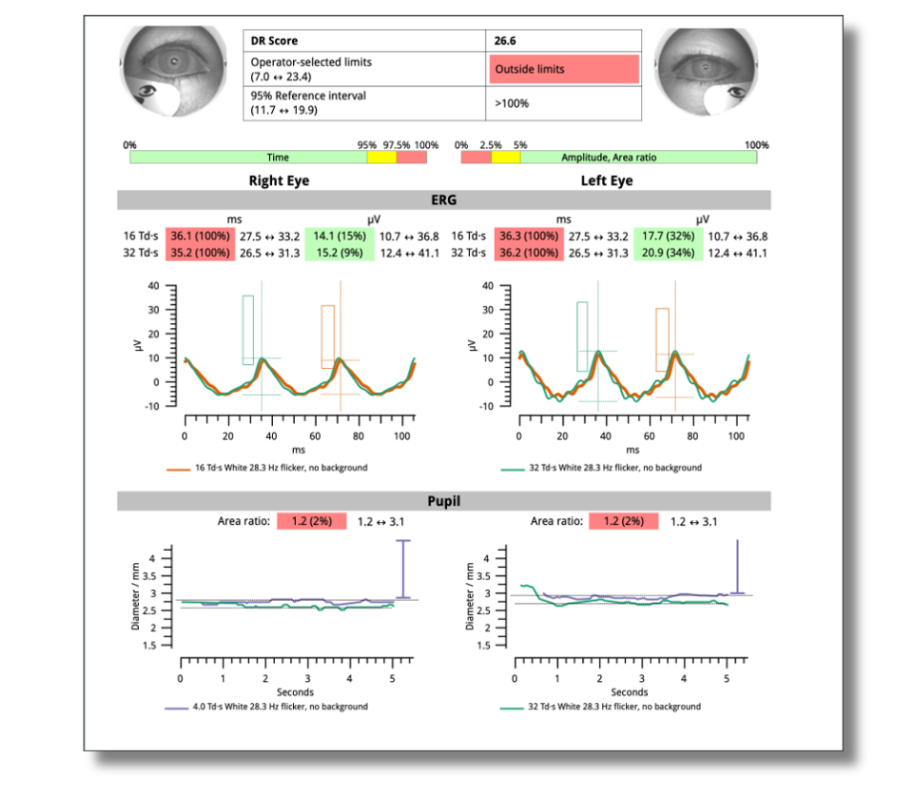
What Were the ERG Findings?
The ERG revealed delayed implicit time in both eyes, indicating cellular stress. Pupil function also was flagged as abnormal, which is not unusual when a patient has significant iris ischemia from long term diabetes. Importantly, the patient had a DR score of 26.6, which is significantly above the 7.0 to 23.4 normal range and can indicate that the patient is at a higher risk of progression within 1 year.
How Did the ERG Impact Next Steps?
Fundus examination was difficult due to dermatochalasis and brunescent cataracts. Based on the ERG, I was expecting to see occlusion, extensive exudates or macular edema, but the retinal function and visible structural findings didn’t seem to match. I did however observe some mild vitreous degeneration, possible mild RPE changes OU, some mild arteriolar narrowing OU, several scattered dot-blot hemes inferiorly, a couple of dot hemes superiorly, and arteriovenous crossings OU. In the periphery, I observed no gross abnormalities OU. The optic nerve head appeared healthy with a cup-to-disc ratio of .30/.30 OU.
Given the high DR Score and the difficulty obtaining a clear fundus view due to dermatochalasis and poor patient cooperation, I referred the patient to a retinal specialist for further evaluation. Approximately two months later, the specialist conducted a fluorescein angiography (FA), which revealed widespread capillary dropout in both eyes—evidence of severe retinal ischemia likely related to the patient’s long-standing diabetes.
This level of ischemia places her at significant risk for developing retinal neovascularization, a hallmark of proliferative diabetic retinopathy. As such, she will now be monitored closely over the coming months for signs of disease progression.
Despite having very few visible structural signs of retinopathy on my examination or previous imaging, the angiographic findings explained that with such severe ischemia and capillary non-perfusion, the retina lacks the perfused vasculature needed to form typical microaneurysms or hemorrhages. This makes detection by slit lamp, OCT, or widefield fundus imaging particularly challenging.
Without ERG testing or FA, the severity of this patient’s condition could have easily been underestimated, leading to potentially catastrophic delays in care. The ERG provided an early red flag when structural imaging failed to convey the extent of dysfunction. It was a key turning point that changed her care trajectory.
Moreover, while cataract surgery may still improve certain visual limitations, the degree of retinal ischemia means that her long-standing complaints of poor night vision are unlikely to resolve entirely.
This case was billed using E11.3293 – type 2 diabetes mellitus with mild non-proliferative diabetic retinopathy without macular edema, bilateral
Why We Use RETeval
We implemented the RETeval device in our group optometry practice in the suburbs of Buffalo, New York, in April 2023. As a medically oriented clinic, we see a high volume of patients with glaucoma, macular degeneration, and diabetes—a population that continues to grow as our patient base ages. With the knowledge that most individuals with diabetes will eventually show signs of retinopathy, we sought out a tool that could enhance our clinical decision-making and improve patient care.
RETeval has done exactly that. It has become an essential part of how we manage diabetic retinopathy—particularly because grading retinopathy based on fundus findings alone can be highly subjective. Determining whether a patient’s disease is stable, improving, or worsening can sometimes feel ambiguous. With RETeval, we now have an objective, quantifiable tool that simplifies these decisions and adds consistency to our assessments.
The DR Score generated by the RETeval ERG provides a clear, functional benchmark that not only guides referral timing and follow-up intervals but also supports patient education. Patients now ask about their DR Score the same way they ask about their intraocular pressure or axial length. That engagement helps reinforce the importance of follow-up and makes conversations about disease status more concrete.
RETeval testing is quick, non-invasive, and technician operated. It’s portable, reliable, and easy for patients to tolerate. For our team, it has delivered greater confidence in determining who can be monitored in-house, who needs a referral, and how urgently intervention is needed—all while improving our ability to connect with and educate the patients we serve.
Practice Protocol
In our clinic, we’ve established a streamlined diagnostic workflow that integrates ERG testing into our daily routine. Each morning, the doctors review the charts for the day and flag which diagnostic tests—such as OCT, visual fields, or ERG—should be performed by our technicians prior to the exam. This proactive approach improves clinic efficiency and ensures we collect the most relevant data before the patient sees the doctor.
ERG testing is performed on most of our patients with diabetes or glaucoma. By incorporating functional testing early in the visit, we’re able to make more informed decisions in a timely manner and minimize delays in diagnosis or follow-up planning. This protocol has allowed us to confidently stratify risk, monitor disease progression, and optimize patient care with greater precision.

Jeffrey Calhoun, OD, FAAO
Advanced Eyecare Center (Williamsville, NY)
Dr. Calhoun is a highly respected optometrist with over two decades of clinical, academic, and leadership experience. A graduate of the Illinois College of Optometry, he completed extensive training through the Illinois Eye Institute and Olympia Fields Osteopathic Hospital. He currently serves as an Adjunct Professor of Clinical Medicine at Daemen University and D’Youville University and is a Fellow of the American Academy of Optometry.