Case study
DR Score Helps Overcome Blind Faith in Popular Weight Loss Drug
by Jeffrey Calhoun, OD, FAAO
Patients with diabetes don’t always comply with prescribed courses of treatment, despite structural abnormalities that threaten their vision – instead, they may rely on medication to control their symptoms. Jeffrey Calhoun, OD, FAAO, an optometrist in Williamsville, NY, utilized his RETeval handheld ERG’s predictive DR Score to educate a patient on his risk of vision loss despite controlling his blood sugar with Ozempic. The patient’s DR Score showed that his worsening retinopathy warranted a referral to an ophthalmologist for further intervention.
Watch the video of Dr. Calhoun presenting his case or review the case below.

Challenge
Assessing Risk for Progression

Diagnosis
Severe Non-Proliferative Diabetic Retinopathy

Testing Protocol
DR Assessment
Patient History
2020
A 46-year-old African American male presented in February 2020 for a routine annual examination. His only complaint was dryness with contact lens wear. His ocular history was significant for high myopia and lattice degeneration OU. He reported an unremarkable systemic history and had not seen a primary care provider in several years. His only medications were over-the-counter vitamins.
Entrance testing was unremarkable. Best-corrected visual acuity was 20/20 OU. Slit lamp examination and intraocular pressure were within normal limits.
Widefield imaging revealed a large optic nerve head with healthy rim tissue OU. However, a cotton wool spot and intraretinal hemorrhage were observed along the superior vascular arcade in the right eye (Figure 1). The left eye was free of retinopathy.
Figure 1: Fundus Exam
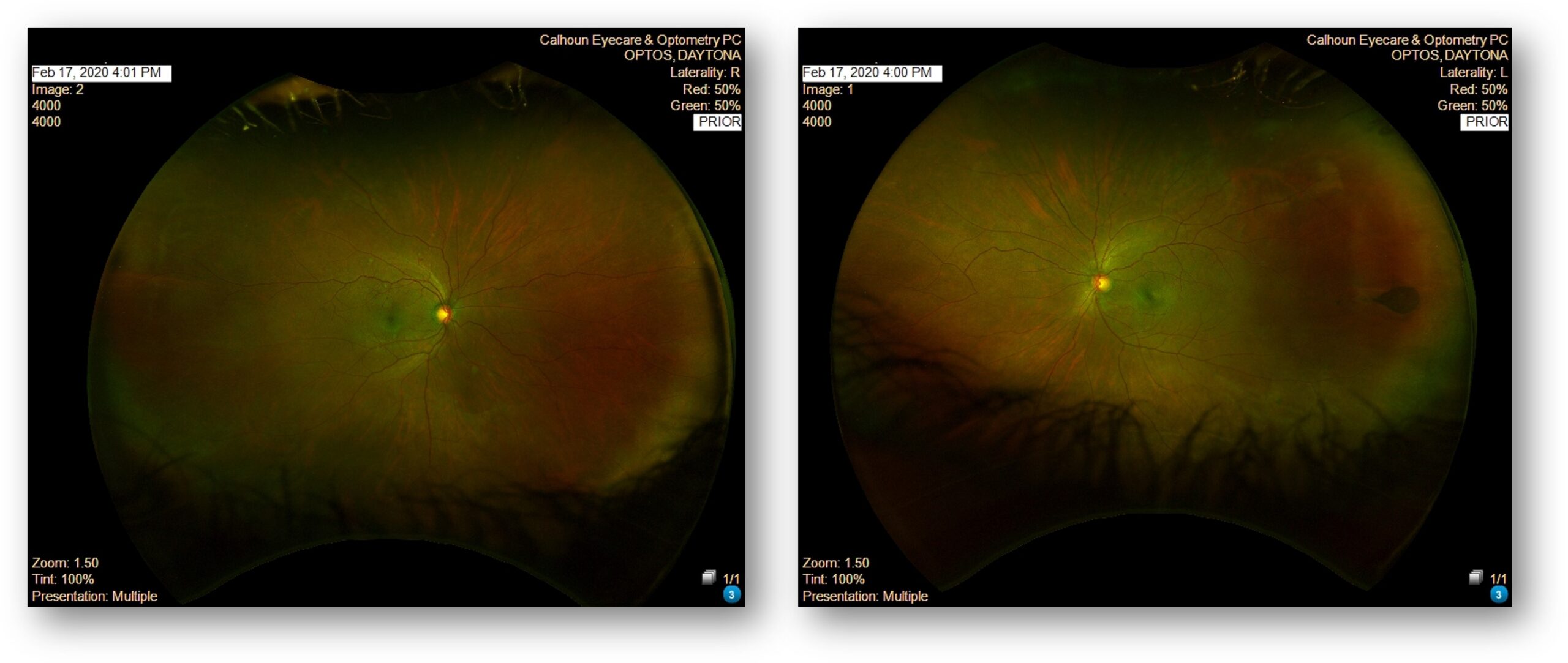
The patient was advised to visit a primary care provider for a comprehensive medical evaluation. Blood pressure measured in-office was 132/82 mmHg. He was instructed to return in four months for monitoring but did not keep his follow-up appointment
2022
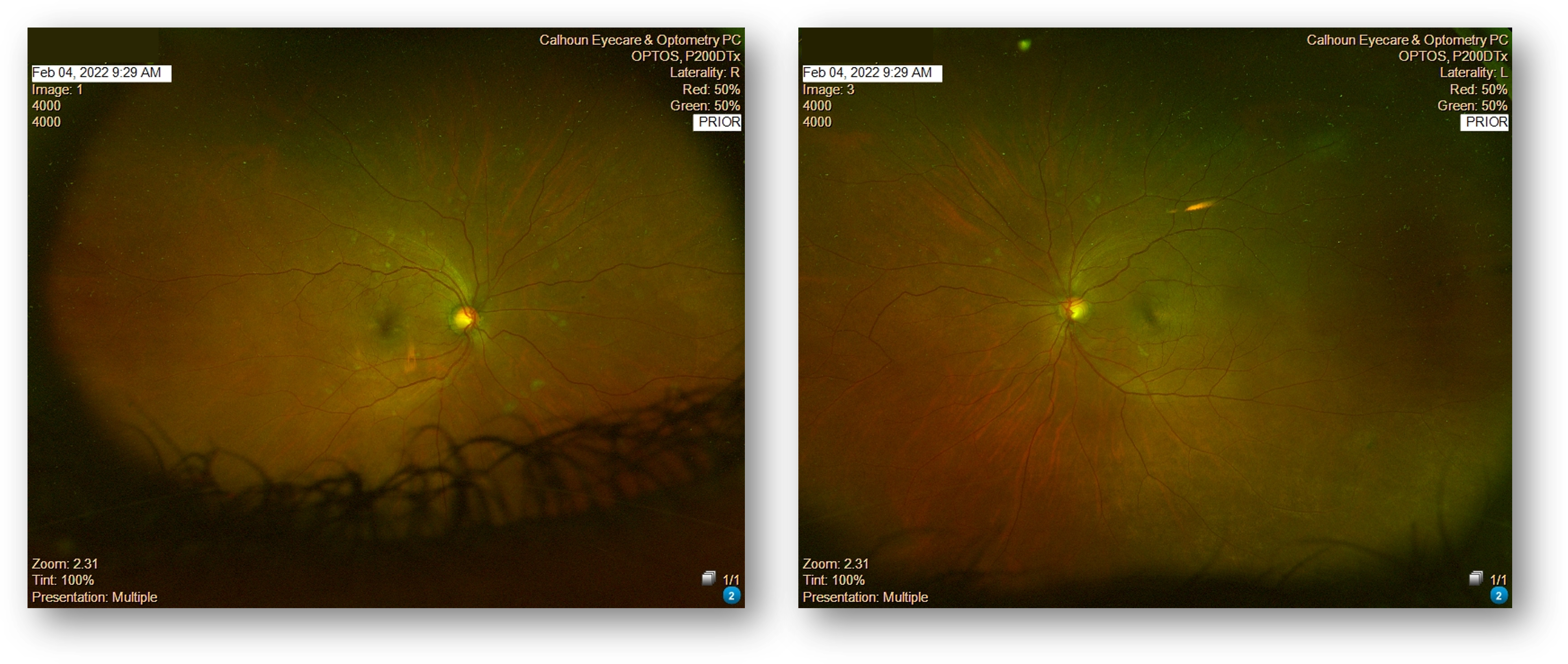
Two years later, the patient returned and reported that he had been diagnosed with type 2 diabetes mellitus and started on metformin. His last A1C was 6.5. Despite reporting good glycemic control, fundus examination revealed worsening cotton wool spots in the right eye and new intraretinal hemorrhages in both eyes (Figure 2). Again, follow-up was recommended.
Figure 2: Fundus Exam
2023
The patient did not return until August 2023. At that visit, he reported discontinuing metformin due to side effects, during which time his A1C rose to 12.0. His physician restarted metformin and initiated semaglutide injections. The patient proudly reported that his A1C had improved to 6.0 and that he had lost a significant amount of weight. He stated that he felt well and believed his retinopathy had resolved.
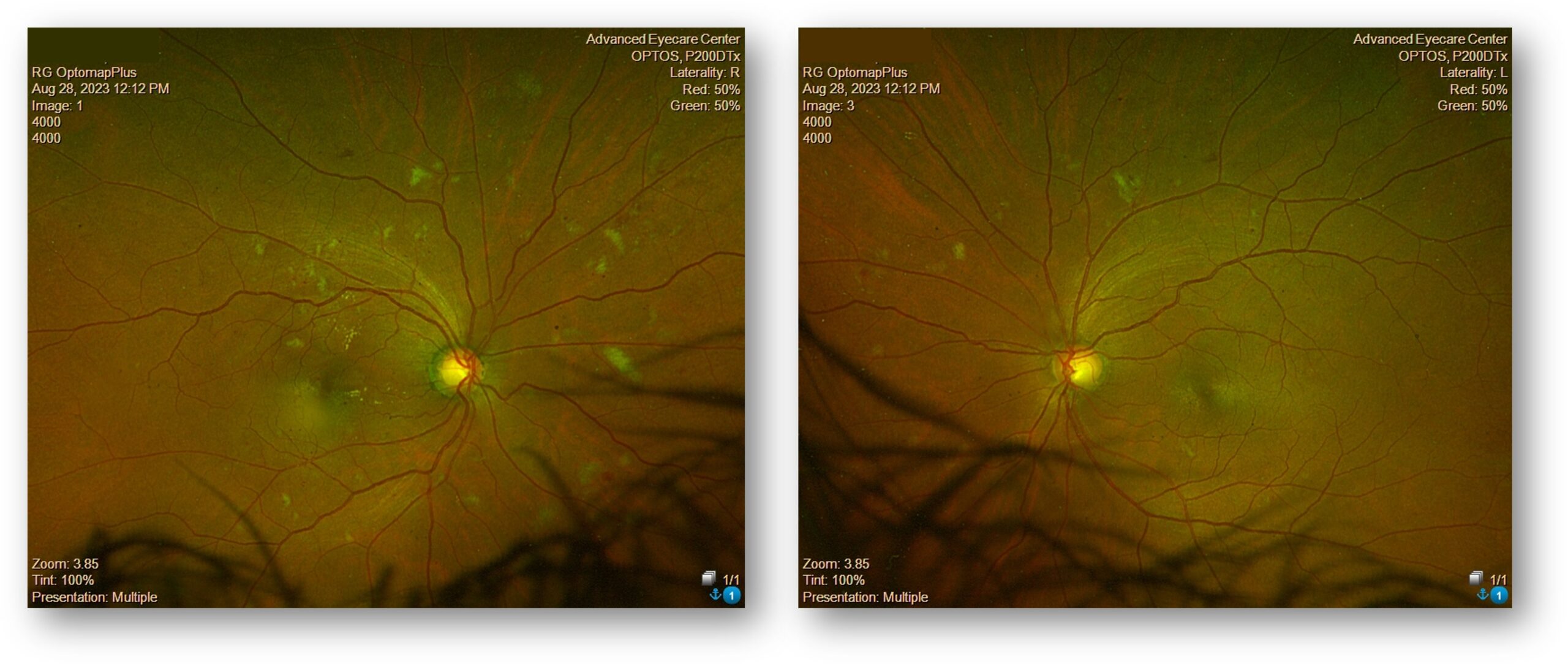
However, fundus examination now revealed dot and blot hemorrhages in all four quadrants OU, increased cotton wool spots OU, and hard exudates near the macula OD (Figure 3).
Figure 3: Fundus Exam
Why Was the ERG Test Performed?
Although the patient’s A1C had improved dramatically and he was asymptomatic, the structural findings had worsened significantly compared to prior visits. The extent of bilateral hemorrhages and cotton wool spots raised concern for progression to severe non-proliferative diabetic retinopathy with possible macular involvement.
Because we now had ERG available, we performed a DR Assessment to objectively quantify the patient’s retinal function. The goal was to determine the degree of retinal stress and assess risk for progression beyond what structural imaging alone could convey.
What Were the ERG Findings?
ERG testing demonstrated severely delayed implicit time OU and significantly reduced amplitude OU. Both parameters were flagged abnormal. The DR Score was 27.6, which is significantly above the normal reference range of 7.0 to 23.4 (Figure 4).
Figure 4: ERG

A DR Score above 26.9 indicates elevated risk – a 79% chance1, in fact – of requiring intervention within the next year. This patient’s score of 27.6 reflected substantial retinal dysfunction and functional stress, consistent with the structural progression observed on imaging.
The objective ERG findings confirmed that despite improved systemic laboratory values, the retina remained under significant stress.
How Did the ERG Impact Next Steps?
Based on the structural findings and elevated DR Score, the diagnosis was revised to severe non-proliferative diabetic retinopathy with possible macular edema OD.
The DR Score played a pivotal role in patient education. Although the patient felt well and believed that improved A1C equated to retinal recovery, the color-coded ERG result provided objective evidence that his retinal function was compromised. Reviewing both before-and-after fundus images and the ERG results helped the patient understand the severity of his condition.
He was referred promptly to a retinal specialist for further evaluation. The specialist identified macular leakage, but not clinically significant macular edema at that time. The patient is now monitored every four to six months.
This case illustrates that rapid improvement in blood glucose control may be associated with temporary worsening of diabetic retinopathy. Structural imaging alone may not fully capture the degree of retinal stress. Functional assessment provided by ERG helped quantify risk, reinforce urgency, and ensure appropriate referral and follow-through.
This case was billed using the following codes:
2020 visit: E11.3391 — Type 2 diabetes mellitus with moderate nonproliferative diabetic retinopathy without macular edema, right eye
- 2022 visit: E11.3393 — Type 2 diabetes mellitus with moderate nonproliferative diabetic retinopathy without macular edema, bilateral
- 2023 visit: E11.3493 — Type 2 diabetes mellitus with severe nonproliferative diabetic retinopathy without macular edema, bilateral
Why We Use RETeval
We implemented RETeval in our group practice in April 2023 to elevate the care we provide for our diabetic and glaucoma patients. Each morning, our doctors review the schedule and determine which diagnostic tests should be performed during pre-testing. This includes retinal imaging, OCT, visual fields, and ERG testing when appropriate.
RETeval provides objective functional data that complements structural imaging. It enhances patient education by allowing us to demonstrate not only what the retina looks like, but how it is functioning. The DR Assessment can be performed on undilated eyes in just a few minutes, improving efficiency while adding valuable clinical information.
Practice Protocol
In our clinic, we perform ERG testing on diabetic patients who have:
- Any degree of structural retinopathy
- Significant changes in systemic control
- Rapid shifts in A1C levels
- Vision complaints inconsistent with imaging
- Diabetes for more than 5 years
Incorporating ERG into our workflow helps us stratify risk, guide referral timing, and reinforce the importance of follow-up care.
1 Davis CQ, Waheed NK, Brigell MG. Predicting Progression to Vision-Threatening Complications in Diabetic Retinopathy. Ophthalmology Science. 2025 Nov-Dec;5(6). DOI: 10.1016/j.xops.2025.100859

Jeffrey Calhoun, OD, FAAO
Advanced Eyecare Center (Williamsville, NY)
Dr. Calhoun is a highly respected optometrist with over two decades of clinical, academic, and leadership experience. A graduate of the Illinois College of Optometry, he completed extensive training through the Illinois Eye Institute and Olympia Fields Osteopathic Hospital. He currently serves as an Adjunct Professor of Clinical Medicine at Daemen University and D’Youville University and is a Fellow of the American Academy of Optometry.