Case study
Using ERG for Management of Birdshot Chorioretinopathy
by Prof. Paulo Eduardo Stanga, Andrea Saladino, William Ayliffe and Sebastian Eduardo Francisco Stanga, The Retina Clinic London, UK
A 62-year-old patient sought a second opinion following a diagnosis of intraocular inflammation in both eyes, which was more severe in the right (BCVA: 0.4 LogMAR) than the left (BCVA: 0.3 LogMAR). An optician diagnosed vitritis. A month later, a local hospital diagnosed the patient with birdshot chorioretinopathy and initiated treatment that included Ozurdex intravitreal therapy in both eyes, oral prednisolone, and methotrexate.
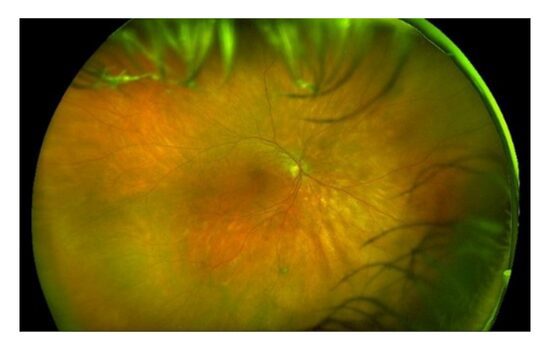
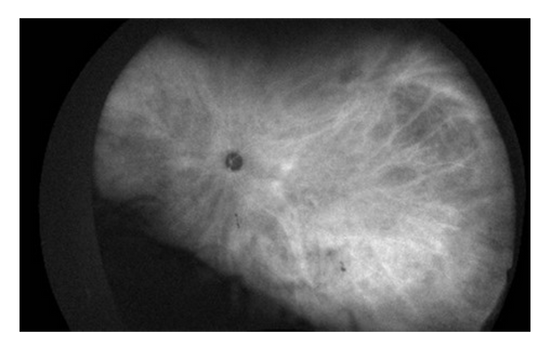
Fundus Color (OD)
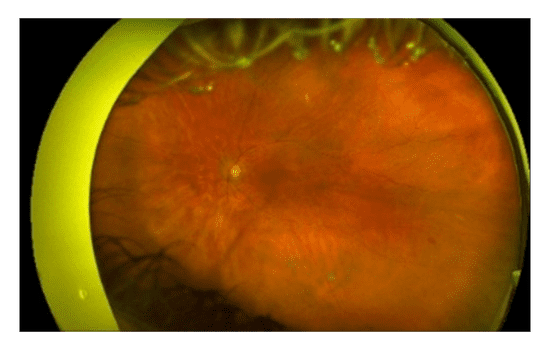
Fundus Color (OS)
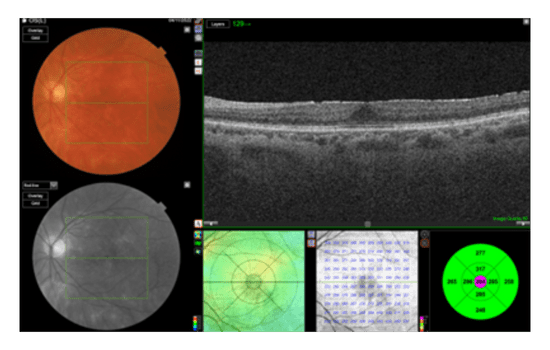
OCT (OD)
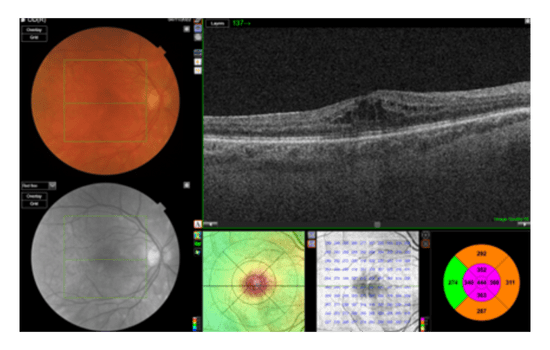
OCT (OS)
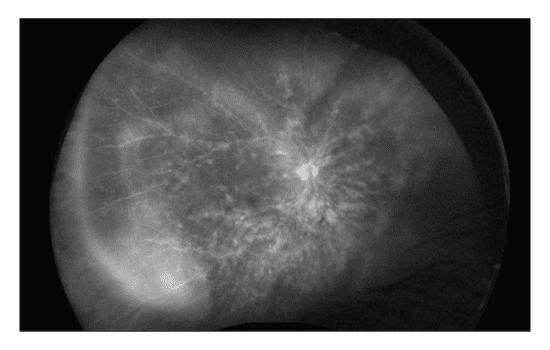
Fluorescein Angiography (OD)

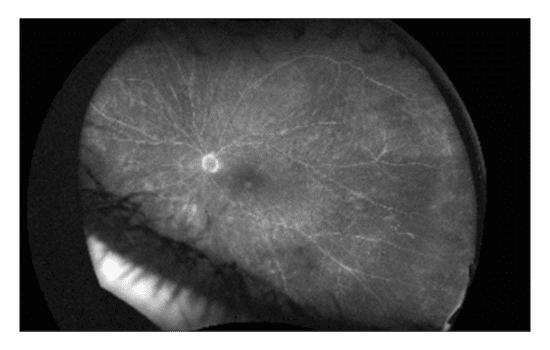
Fluorescein Angiography (OS)

Challenge
Determining appropriate treatment plan

Diagnosis
Birdshot chorioretinopathy

Type of protocol
Flicker: 32 Td·s
Why was the ERG test performed?
Despite several multimodal and ultra widefield images, there was a need to obtain objective functional data to assess if active inflammation was still present from the birdshot chorioretinopathy. If so, what was the extent of the inflammation? Since treatment had already started, the RETeval® ERG was needed as an objective biomarker to further define the type and amount of treatment.
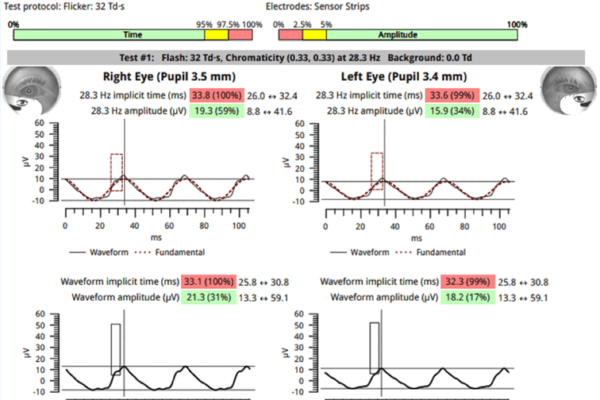
What were the findings?
ERG results from the Flicker: 32 Td·s protocol showed increased implicit times outside of the normal range which confirmed the presence of widespread retinal inflammation. Despite ongoing treatment, the implicit time was still delayed, indicating the need to adjust the treatment plan.
How did the ERG influence the patient’s care?
Further immunosuppressants were prescribed as the inflammation appeared to be active and severe in the affected area. Additionally, the prednisolone was tapered in 1mg steps per week from 10mg until it reached 5mg a day.
Conclusion
The use of ERG in this case helped to determine the optimal treatment plan and schedule for the patient. The delayed implicit time, indicating active inflammation, prompted an adjustment of the patient’s medication to reduce the inflammation quickly and effectively.

Prof. Paulo Eduardo Stanga
The Retina Clinic, London, UK
Professor Stanga is the Founder and Chief Medical Officer at The Retina Clinic London, and Professor at the UCL Institute of Ophthalmology. With over 30 years’ experience in Ophthalmology and a focus on Medical and Surgical Retina, including Macular Degeneration, Diabetic Retinopathy, Vitreous Floaters, Cataracts, Retinal Laser, R&D New Therapies, Surgical Technology, Advanced Imaging & Clinical Studies, Prof. Stanga is committed to advancing the realm of eye care and is dedicated to transforming lives through pioneering work in Ophthalmology. Dr. Andrea Saladino, Prof. William Ayliffe and Mr. Sebastian Stanga have all been instrumental in the care of this patient. The Retina Clinic London is focused on delivering bespoke eyecare.